celt262 wrote: » What medicine should be taken if symptoms start to develop?
dartboardio wrote: » Hi, Do you find yourself turning away lots of patients who don't have any real symptoms of the virus and are just taking up waiting rooms out of worry? Are all your staff/colleagues full of panic/worry ? Is this the busiest you have ever been?
expectationlost wrote: » is it possible to protect yourself from the covid19 and treat patients, how are health workers still getting sick?, are not wearing some level protection now?
TheValeyard wrote: » Are there still the usual cough, colds, flu going around that could also be affecting people. If my toddler has a runny nose and slight cough, it's not immediately Covid19 but still the usual suspects?
JP Liz V1 wrote: » I have so many questions, where to start as an asthma sufferer ( and nothing on line ) how do you differentiate between an asthma attack or Covid19?
banie01 wrote: » Do you think that our effort to shift the curve and flatten growth will be successful?
banie01 wrote: » Or that we took our measures a week or 2 too late for maximum efficacy?
CtevenSrowder wrote: » How long do you think the lockdowns will be required to last?
CtevenSrowder wrote: » Why is it presumed that warm weather will reduce the number of cases?
sgthighway wrote: » What is your speciality?
History Queen wrote: » Have ye received any further guidance regarding coronavirus and pregnancy? Specifically the case in the UK where the newborn tested positive for the virus, has that changed anything regarding the treatment/guidance for dealing with pregnancy?
coastwatch wrote: » No question yet, but just to say a sincere Thank You to all HSE staff, frontline and support for the huge effort that has gone into the preparations for the spread of this virus, and for the ongoing effort that will be required to deal with it over the coming months.
humberklog wrote: » Whenever my mate is asked what he does for a living he says "Doctor". He's an Ed. D (Dr. of Education) and does indeed work in this field (Adult education). Does it get your goat when you hear people claiming to be a doctor when their field is non med/psych?
Damien360 wrote: » Serious question. What would be your honest opinion of the current trolley watch numbers ? Why have they collapsed ? People didn't suddenly not require A&E or are the vast majority of A&E overblown ? Figures before Covid-19 over 300. Last year same time 180. This week reported as zero. And thank you for putting yourselves in the way of harm to deal with this. It cannot be easy for your families.
Darwin wrote: » First off, sincere thanks and respect to you and all your colleagues for working at the coal face in these unprecedented times. My brother is to be tested for covid19 shortly, I wouldn’t expect him to be in the severe risk category. I’ve read of non acute cases that develop ‘mild’ pneumonia. Can this category of patient recover at home without intervention?
Boulevardier wrote: » A friend is having a small dinner party (4 in total) at her home tomorrow night. Is this contrary to current HSE advice? BTW I don't understand where the answers are. I will try again.
ironwalk wrote: » Much respect and gratitude to all the doctors, nurses, ambulance personnel, in-hospital cleaners, admin staff, radiographers, porters, med lab scientists, etc etc. All putting yourselves in the firing line, mentally and physically. The vast majority of the public understands this....but you are more likely to hear from the terrified few who will shout at you. Have you heard from your colleagues in Italy? and did the HSE start to ramp up capacity in line with the warnings that were coming from there last week?
ironwalk wrote: » and did the HSE start to ramp up capacity in line with the warnings that were coming from there last week?
Boulevardier wrote: » Not sure what is going on here. I have been several times now on the "answers thread" and there is nothing there.
begbysback wrote: » Is vitamin D really any good as a prevention of the virus, niacin in particular.
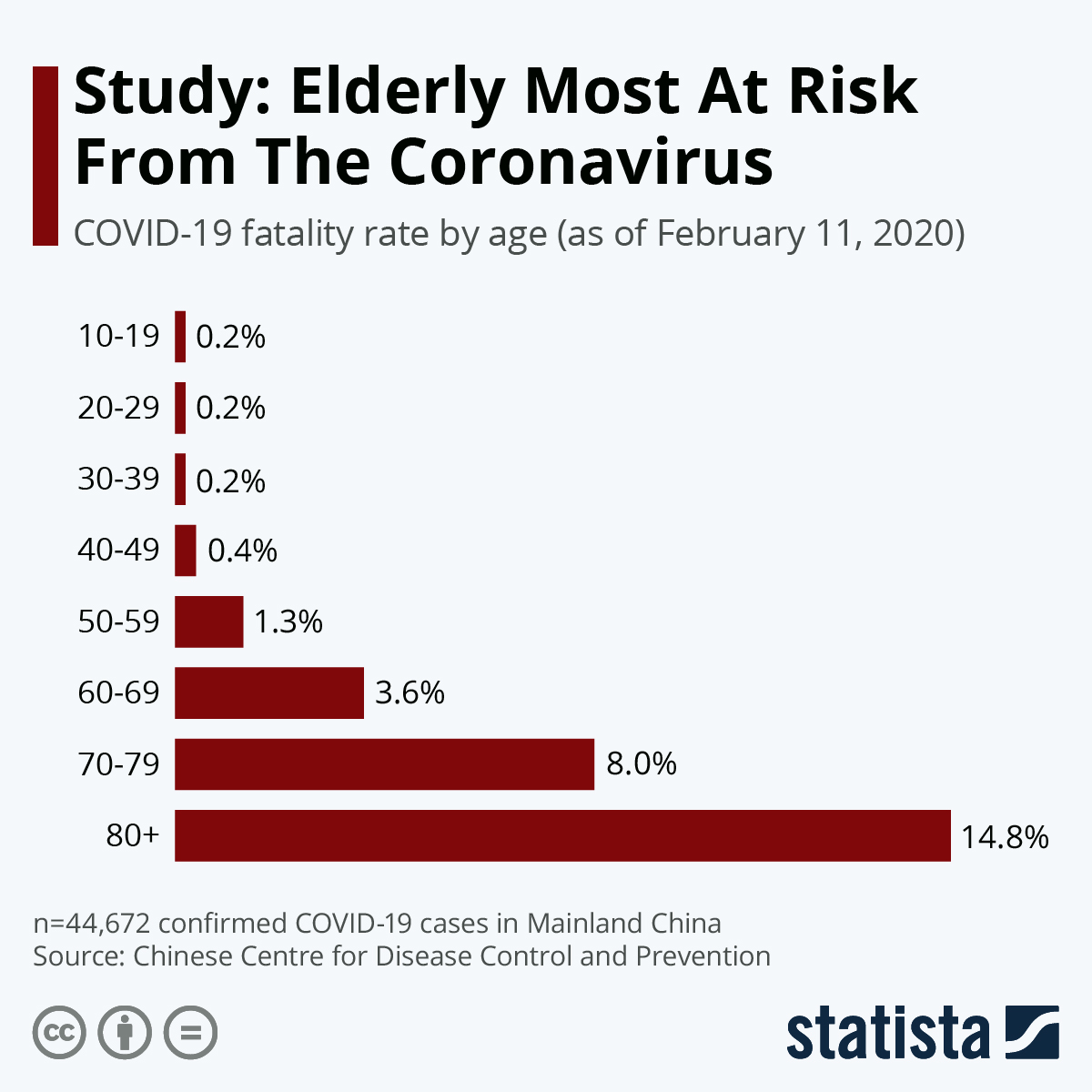
little bess wrote: » The Uk are asking over 70’s to self isolate, would you recommend the same thing to that age group here?
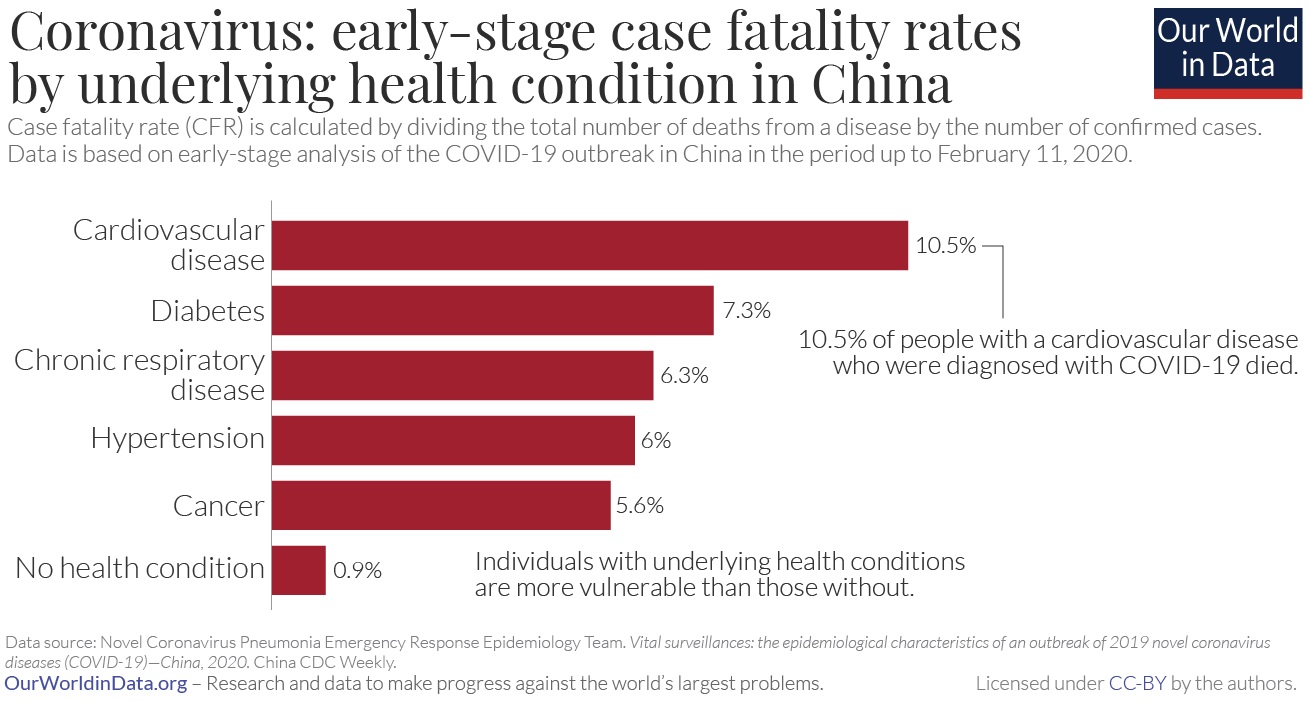
little bess wrote: » I’ve heard diabetes, hypertension, copd are all extra risk factors, should these people take more care with social distancing? Many Thanks
Gloomtastic! wrote: » What’s the difference between a bad dose of the flu and Covid-19?
patsy_mccabe wrote: » If someone gets the virus, get sick and get well again, at what point can they be confident that they have stopped shedding the virus?
KKV wrote: » To re-word it, how are you managing to get time to do a Q+A on here? Has your actual working day/week changed with the virus? Or are ye folks still working the same hours, albeit arguably with more to do during those hours? Or has the trolley crisis suddenly getting solved actually meant that your working day is easier than it was before the virus became so known?
KKV wrote: » Has your actual working day/week changed with the virus? Or are ye folks still working the same hours, albeit arguably with more to do during those hours?
KKV wrote: » Or has the trolley crisis suddenly getting solved actually meant that your working day is easier than it was before the virus became so known?
dharma200 wrote: » All my Chinese students families have been wearing masks at home at all times. They take the masks off for bed. The children ( my students) do not wear masks. They have emphatically told me over and over again to wear a mask, at all times. That this is the success against the virus. I have been seeing my parents with masks on now for five weeks. At home. I am wondering why the advice here is not to wear masks. is it that it is a false sense of security? My chinese families do not understand why everyone here in the west is not being told to wear a mask. Thanks,
PaybackPayroll wrote: » 1. Do a proportion of people who recover have permanent lung damage?
PaybackPayroll wrote: » 2. Is the Irish strategy to get 60% of people infected and recovered, but at a steady rate so a not to overwhelm the HSE, or is there some other strategy?
PaybackPayroll wrote: » 3. Roughly, how long does each phase of the illness last?
PaybackPayroll wrote: » 4. What is the current ICU capacity, and is this being massively ramped up?
PaybackPayroll wrote: » Thank you for taking the time to do this AMA, and also for all of your efforts in tackling this horror.
Day Lewin wrote: » Is this rumour true, that anti-inflammatories like aspirin and Nurofen make you more prone to the virus?
celt262 wrote: » Just seen this pic online. Does it frustrate you that people are making up stuff and posting on social media?
Scot_in_Dublin wrote: » Not a question, just a very sincere thank you to you and all of your colleagues globally who are working around the clock to keep the rest of us going.
YFlyer wrote: » Can you explain the 15 minute in contact time?
Ladybird18 wrote: » My child who is asthmatic is complaining with sore throat and nausea tonight. Should I be worried?
Fann Linn wrote: » What happens after you've self isolated for the 14 days after testing positive? Have you built up an immuninty? Could you catch it again? And a big well done to all in emergency services and the HSE.
Fann Linn wrote: » Have you built up an immuninty? Could you catch it again?
LuckyLloyd wrote: » Best of luck over the coming days, weeks and months. Are the HSE trying experimental treatments ala South Korea and China? I'm referencing chloroquine here and some of the old HIV drugs that have been mentioned.
Andrew H wrote: » I work in the public service as a Clerical Officer and there are rumours that we will be sent home on Friday. Is there any way I can volunteer to help out?
Drumpot wrote: » Can I ask if it’s true that “mile symptoms” can actually be like a nasty pneumonia, so while it’s medically mild it could really knock people back?
Drumpot wrote: » At what stage should a person contact the emergency services for help? What fever in adult and if they find it hard to breath?
Drumpot wrote: » Would keeping track of BP and Oxegen levels help emergency services decide whether you need hospitalisation? (Oximeter readings)
Drumpot wrote: » Asides from being tested will a lot of people with “mild symptoms” possibly not ever know that they had the disease unless for some reason they are tested? Is it possible in the future to be tested to see if you had it or have antibodies?
messinkiapina wrote: » For individuals who experience mild symptoms to the point they may not even know they've contracted it (and presumably develop immunity afterwards), will testing be available to them at some stage? And would those tests show that the virus had been present but overcome? It would be ideal if everyone who's had this knew about it, they could stop social distancing and help the vulnerable and those in need of care?
sadie1502 wrote: » Drugs to treat malaria and arthritis have been showing positive signs in treatment. Will these be available in Ireland if required? Thank you for your help in uncharted territories. Keep safe.
Cork Boy 53 wrote: » I am just curious as to whether you think a time may come when a virus or some type of infectious disease will appear that will have the potential to effectively wipe out all of humanity. I`m talking 12 Monkeys style here. Hopefully this one won`t be it! Anyway my thoughts and prayers are with you and your colleagues for the ordeal that lays ahead of you.
Funnyonion79 wrote: » My question is this...in two weeks time, after self isolating at home with my husband and children, is it safe for us to visit my parents/in-laws, who have also been self isolating at home, during this time? The only time any of us would've left the house is to go for a walk or go to the supermarket. The in-laws are mid 70s but in good health.
JustAThought wrote: » Still wondering where the answers are, please - is there a link? Q: While front line staff paid are being allowed home on paid sick leave inc to mind their children off school unpaid inexperienced volunteers are being emailed from the HSE asking them to go into hospitals to help with the virus. Something fundamentally wrong with this. Surely the time for paid HSE staff to pull their weight is when there is a crisis and they are needed and not be asking or relying on emailing randomers from a charity database to pick up their slack. My family member called in sick on full HSE pay to mind her children - surely this type of abuse should be stopped.
irishgeo wrote: » How long is the recovery period?
Seamai wrote: » What is the protocol if a work colleague tests positive? Is the work place contacted? and if so by who? What happens after that?
JoChervil wrote: » It was a disease running around late December/early January. In reports from that time it was said that there was a 25% increase in hospital admissions of patients over 75. So my question is: how HSE ruled out that it was not Covid-19? How many tests were made to prove it was something else like a different kind of flu (I mean percentage of cases checked for it)?
piplip87 wrote: » Hi there, Have you seen any day services cancelled ? My OH has MS and is on a monthly infusion. As far as I understand there is a massive increase in the risk of an attack if left for more than 5 weeks between treatments. Have you seen or heard if any alternative arrangements for these treatments ?
Kerry25x wrote: » How do you feel about the speculation happening that health care workers are at much higher risk of developing severe/critical illness if they come infected? Have you any advice for other front line hospital staff?
laserlad2010 wrote: » If you're not a public health specialist you have no business providing official COVID-19 advice, even cloaked as personal advice, to the public. It's bad enough with the Whatsapp rumours, but talking about writing your own will at the same time as attempting to give advice in your capacity as a consultant is inapproriate. Regardless of whether it turns into a "war". Even if you claim you're not representing the HSE people will still place weight on your words.
Balf wrote: » Maybe we should ask him if threats like Covid 19 show the impracticality of organising access to medical knowledge through a tiny bunch of highly paid consultants. I think he'll know what we mean.
Agus wrote: » Thanks for taking the time to do this, I think it really helps to have good information out there as much as possible. 1. How soon do you think the number of infected people in Ireland who need treatment will reach a level where the health service is finding it hard to treat them all?
Agus wrote: » 2. I've seen reports that asthma may be a risk factor because Covid might exacerbate the asthma, but the actual Covid illness itself isn't necessarily more severe. In other words, the claim is that the main extra risk to people with asthma is that they will end up with both Covid illness & a severe exacerbation of the asthma, and therefore the additional risk for people with mild asthma is probably not much greater than people without asthma. Is this likely to be accurate or not?
Sour Lemonz wrote: » My eldest nephew (age 11) has cystic fibrosis, my sister does all his IV's at home, he is on orkambi, lung capacity up and all good stuff at the moment. However with the virus going around there is obviously a concern for him as lung functionality could become an issue. He is very good at washing hands and looking after himself like meds for his age, but there are going to be times where he cant control a situation and may pick this virus up. Some advice that was given to me today (cant confirm person is a health professional) was that if my nephew showed symptoms then get him to a sauna 2-4 times a week for 30 mins at a time that and the heat and steam of the sauna would kill the virus as it lodges in eyeducts, nasal cavity. Is there any truth to this ?
tatranska wrote: » I watching a UK parliament committee asking about the lack of appropriate PPE for medical staff on the front line of the NHS. How are medical staff fixed for safety equipment in treating patients.
Fishorsealant wrote: » What do you think of the situation regarding dentists? One of the professions most at risk yet very little guidance available. One of the last professions to be considered despite providing an essential role and being at high risk. Many dentists taking it on their own to decide whether to open or close. Do you think forced closure except for emergency treatment would be wise?
Away With The Fairies wrote: » Keep hearing that the majority of people will get through this fine at home? Do we ring doctor on day 1 just to make them aware that you're not feeling the best?
locohobo wrote: » No questions..Just to say well done to you and you're fellow front line staff.... From the description you gave of you're own self imposed current isolated lifestyle it should be enough to make people aware as to just how serious this threat is.. Myself:- Legionnaires disease 10/'19...COPD..Smoker...SO I realise the limitations of my survival through this and have already come to terms with it..will not be expecting to tie up an incubator....
Multipass wrote: » Thank you so much, it’s great to have so much information in one place. I’m just wondering, as A & Es become overwhelmed with this - will there be seperate areas for people coming in with other problems. Thinking of elderly parents having middle of the night heart symptoms or similar. Would letting people wait in cars be an option?
AndrewJRenko wrote: » Thanks for your inputs, very helpful, and thanks for your ongoing work. What's your understanding of the risk of outdoor activities, particularly for teenagers? Is there risk arising from a brisk walk, or a chat at a picnic table outdoors? Mental health is a real concern, and they do need to have some contacts outside the family circle.
mrsherself wrote: » Hi! I was just wondering - I know best advice is to stay inside, but for those of us who will end up going mad, is there anything wrong with going for a walk outside by yourself? Is it not a good idea to go to a park where there will be other people?
malpas wrote: » My wife and I are in our late 60's. She has well controlled bronchiectasis for c.5 years and I was hospitalised and successfully treated for septicaemia around then also. No major issues, both in good health and walk daily. Would either condition mean a greater risk of complications if we got infected? We are taking all recommended precautions and don't expect a medical opinion, just any general views you feel you can offer.
Sober Crappy Chemis wrote: » Realistically, is it a big risk to go to a supermarket or pharmacy obeying physical distance etc, if one has asthma and is also immunosuppressed?
Damien360 wrote: » This question and answer thread(s) has taken me completely away from the main rumour and conjecture thread. It has done wonders for my well being with regards to worry. Yes I know it’s coming and unavoidable but the main thread lacks the sanity in these.
Olaz wrote: » Thank you for your informative and reassuring answers so far. What is your opinion of small children (aged 5-9ish) playing together in small groups on driveways/on the road while doing their very best to maintain social distancing; children who play together everyday and who, under normal circumstances, are in and out of each others houses almost everyday. They wash their hands immediately after coming in, and door handles etc are cleaned regularly throughout the day. Are they putting us, their parents, at risk? They are isolated from everyone other than their own parents and those few pals. Is this behaviour potentially speeding up the spread?
up for anything wrote: » I met a friend I haven't seen for a couple of years the other day. We were chatting about our children, one 'stranded' on a Spanish island and mine just home. I asked her kind of tongue in cheek about what her husband, a fairly senior detective locally, and his colleagues thought of the whole Covid-19 'business'. She replied that his job description had been changed to one thing, just the one thing. When I asked her what, she replied, "transporting dead bodies". From what the undertakers were told and from general knowledge I know that the bodies of those who die of Covid-19 will be hastened to the crematorium and into the ground as quickly as possible and will need people to be responsible for the process. However, the way she said it and the look on her face seemed to say volumes. Are you expecting many people to die in the next couple of months and what is the figure? I assume a figure must be available from the data from other countries and applied to Ireland. Morbid question, I know.
up for anything wrote: » Oh, another question, if you don't mind. People with Diabetes are very much at risk apparently. Is it more those with Type 1 or those with Type 2 or those who have Diabetes which needs to be treated with insulin rather than Metformin/exercise/diet. Are Type 2s with just over the borderline sugar levels, more at risk than someone without it. If you're not sure, would you be able to point me in the direction of some information please and thanks?
Gentleman Off The Pitch wrote: » There are reports of people successfully overcoming the fever after a few days, only for them to be hit with severe shortness of breath and pneumonia a few days after that again. Are there are warning signs of this occurring and are there specific instructions for people who suddenly find themselves in that position, particularly those in the at risk category, so that they make the correct decisions and attempt to get appropriate help as soon as possible?
AidenL wrote: » On underlying conditions - I have had a heart bypass, 10 years ago, 54 now, in good shape generally, did a 13 minute treadmill test a month ago and had follow up with cardiologist in Mater. Hit 100% max heart rate, etc, so cardiologist was happy with the performance. Just wondering if a bypass fixed the heart issue, is CVD still a reason to self isolate when the time comes with my underlying condition? Am I at the same risk as someone with COPD, heart failure etc, or can I go about my business? I know the bypass fixed the problem, and the disease still exists. Hence my question, mortality rate for CVD is quite high, seemingly 13%, so I have that concern of course. Thanks in advance.
Simdruid wrote: » Many thanks for both this thread, and all the work you are going to be doing over the next period of time. Stay safe. For those of us with underlying conditions, with regard to Leo's speech last night, he mentioned elderly and vulnerable and cocooning. Do you have any idea how we are going to identify whether our underlying condition is sufficiently risky to warrant this when we are not elderly?
beolight wrote: » Asking for a friend ��...There’s lots of us here with partners working in the healthcare system ( me included) What precautions do you take or recommend when coming home from work to protect your own family
DevilsHaircut wrote: » Should we be making it completely and unambiguously clear that SELF-medicating with anything for Covid19 symptoms will do nothing to fight the actual virus?https://www.boards.ie/vbulletin/showpost.php?p=112861398&postcount=5158
banie01 wrote: » Hi again Psuedo, just a question that came up over on the Diabetes thread. As Diabetics are a high risk group as per the advice from Government/WHO, many of us are taking all available precautions. is there however any difference in the advice for T1 and T2? Or is it a blanket advice? My own understanding of T1.5, T2 in particular is that as inflammation is a particular risk in any event that it should be a case of isolate and stay safe? Does one's control have any bearing? or is it really a case of suck it up, mitigate and isolate?
celticWario wrote: » In relation to claims by a HSE whistleblower that the current state of hospitals are "filthy", has there been an effort to deep clean our hospitals in the past few weeks in preparation for what's to come?https://www.dublinlive.ie/news/dublin-news/coronavirus-filthy-hospitals-wont-able-17884118
mariaalice wrote: » If someone suspects they have the virus but are generally well and have painkillers at home and they decide to stay at home for two weeks and just get through it. Do they need to get tested or can they just stay at home?
Yester wrote: » How can we help? At the moment we are taking this seriously and avoiding all unnecessary contact with others. We do ring older people to see if they need anything but they have been ok so far. When things get worse, will there be volunteers needed or is continuing to isolate the best thing we can do? Edit: Do you think things like this interactive map connecting volunteers with the self-isolated are a good idea?https://www.limerickleader.ie/news/community/526492/interactive-map-connects-volunteers-with-self-isolated-in-limerick-during-covid-19-crisis.html
Goldenkt wrote: » Quick question regarding self-quarantine, should someone whos in remission from hodgkins lymphoma for just over a year and received 6 months of ABVD chemo be travelling into work on public transport & work in a busy office in the city centre or do they fall under the at risk group advised by HSE to self-quarantine?
Call me Al wrote: » Thank you for your guidance, and the work you and your colleagues will be doing. Your last post said this: "It is just a matter of time. Buy us that time with social distancing, social isolation and handwashing." Do you think we are doing enough? My household is doing absolutely everything by the book but its frustrating as hell when I heard about people going to house parties last night and kids like my own on playdates who are all unable to self-regulate the social distancing. I called my health insurer nurseline about information I'd read, (both media and scientific journals) about ace inhibitors and concerns surrounding these. I was told that their medical teams were aware of this and that there were many uncertainties. Now I'm not coming off the medication or anything extreme like that, and I did contact my gp with my questions, which we all should do! Is there any verifiable science surrounding these medications and their interactions with covid19?
RiseAbove4 wrote: » I’ve been reading your posts with both interest and high anxiety. I believe all your facts and thank you for doing this. Question: I’m a 44 year old male with Cerebral Palsy. In addition I’ve early Osteopenia and I’ve picked up some kidney stones in the last couple of years. I’m also allergic to Penicillin which is used to fight off lots of bugs. . My CP is mild compared to others. I can still walk and I try to exercise as much as possible. Am I at any higher a risk than another 44 year old male? I’ve been distancing myself from most people for about 10 days now and I’m going to focus on looking after my immunity with high dosage Vitamin C, Zinc and more. Cheers again.
faceman wrote: » As the Americans say to the veterans, “thank you for your service sir” My question is probably more complex than I think but here goes Viral loads and contagions. How does it work with this virus. We know that there are drugs for example that can suppress viral loads of HIV to levels that make it virtually not transmittable. What is it that makes this virus so contagious? Is it it’s ability to replicate itself? Or have I oversimplified it?
Imreoir2 wrote: » Is there a reason for the high mortality rate experianced in Italy to date as compared to other countries?
The One Doctor wrote: » No questions, just thank you for your forthrightness, bravery and determination. If we ever meet, I will buy you a beer. Several beers.
Drumpot wrote: » https://journals.lww.com/ajg/Documents/COVID_Digestive_Symptoms_AJG_Preproof.pdf ————————————————- Conclusion: We found that digestive symptoms are common in patients with COVID-19. Moreover, these patients have a longer time from onset to admission and their prognosis is worse than patients without digestive symptoms. Clinicians should recognize that digestive symptoms, such as diarrhea, may be a presenting feature of COVID-19, and that the index of suspicion may need to be raised earlier in at-risk patients presenting with digestive symptoms rather than waiting for respiratory symptoms to emerge. However, further large sample studies are needed to confirm these findings. —————————————————- There are some reports that Gastro problems (like diarrhoea) can be an advance warning and in a small study of Hubei patients, just under 50% had this as their primary symptom. Have you heard anything regarding this or is there any sign that this has been a symptom from what you have seen thus far? Thanks for answering all these questions, it really helps...
Standman wrote: » I'm a bit confused about the advice regarding hygiene/social distancing - HSE website says masks are unlikely to be effective for healthy people and seems to advise against gloves, but you reckon it's irresponsible to go to a supermarket without gloves and masks? Also, if we're worried about touching surfaces in a supermarket then what about the things we buy and take home? Should we be disinfecting packaging? Thanks.
Skygord wrote: » My wife finished chemotherapy 6 months ago, and had a splenectomy 3.5 years ago. We understand she is in an at risk group. Are there any extra precautions that we should follow - over and above the guidelines for self-isolation?
Drumpot wrote: » My sister smokes but had leukemia when she was a child. ( not had problems or check ups in decades). She works in a hospital up north and when I asked her if she had spoken to a doctor about her risk factor she said she didn’t see it being a problem. She’s also refusing to buy these personalized masks they are offering. Would a person who has , I think, fully recovered from this illness theoretically not be anymore at risk then the average person? I appreciate you cannot give medical advice here, I am just wondering how insistent I should be with my sister that she should talk to a doctor regarding her risk profile, especially while she’s working in a hospital....
Fluorescence wrote: » Thank you for taking the time to answer the questions, and for continuing to work despite being at considerable risk. This really is a war. I work in the veterinary sector. Many of our clinics and hospitals have ventilators. In the UK, the AHT is compiling a list of veterinary ventilators and liasing with officials to coordinate their potential donation/use in the hospitals in the weeks to come. I don't know if the Irish bodies are aware that these facilities may be available to draw upon? It's not a standard piece of kit in every hospital but there are many around, which may be worth investigating. Aside from ventilators, is there anything veterinary staff in particular can do to assist in the coming crisis?
Hobgoblin11 wrote: » Is sex ok during this crisis or should we be avoiding that also? When can we go back to this type of thing if it's not recommended? Do you contact trace your partner?
17-pdr wrote: » I see that having high blood pressure is one of the risk factors. If you are on medication for it and your BP is now ok, is an underlying risk still there?
Arlessienne wrote: » In your opinion, how high risk is someone (aged 40) with Inappropriate Sinus Tachycardia requiring 7.5mg bisoprolol daily and suffering fairly significant exercise intolerance? They are an ex medical scientist and looking to volunteer - is their risk of further burdening the health service if they get sick low enough to go ahead? It's impossible to get any response at the moment from gp or cardiologist. Obviously this would be just your theoretical opinion on this condition generally, without knowing full details. Thanks for all you are doing both in the hospital and in spreading awareness here. Your posts are scary but I believe them to be realistic. Thanks for trying to get people to wake up to reality.
lillycakes2 wrote: » I am a nurse, I live with my mum who is over 70,self caring. I am not going near her, I am using just one room (my bedroom), with door closed, I am using my own toilet, my own cutlery and I just walk out front door when I go to work, she is not allowed to use this door , she uses the back door.i am not using any room in the house ,I am showering etc in work.... Does this sound ok to you ?.
supermouse wrote: » Firstly, thank you for doing this AMA. Furthermore, thank you so very much for everything you have done to date and will no doubt continue to do well into the future to protect us all. Why do you think we haven’t been put in lockdown yet? As we’ve all heard and seen, social distancing is working for some but so many are ignoring the rules. Mr Varadkar has access to the same data as you, is a medical doctor himself and is surrounded by some of the brightest minds we have in this country. Why are we delaying the inevitable do you think? Stay safe. I truly mean that.
Whiplashy wrote: » I live with my elderly parents and I myself am on weekly benepali injections. When the government recommends cocooning, would I need to follow that recommendation as well as my parents? We live in the country with no family nearby so would need to be thinking about trying to put arrangements in place if necessary.
Xertz wrote: » A genuine question, and I know it might be impossible to answer, but do you foresee this going on for a few months or are we looking at a new normal well into 2021?
Arlessienne wrote: » Thanks so much for your response. It was very helpful. I will pass on your advice about volunteering for a role with no or little contact and he will hopefully eventually get a specific response too from one of his doctors to be safe. (IST is the official diagnosis written in medical reports from a cardiologist specialising in electrophysiology and was deemed to be a type of SVT and possibly a form of dysautonomia or SA node malfunction.) Best of luck and thanks to you and all your colleagues.
up for anything wrote: » Based on our figures today, 20th March, and the lack of proper social distancing going on, what do you think our best, medium and worst case scenarios are going to be regarding deaths?
up for anything wrote: » Are there going to be enough ventilators, do you reckon, for say the medium case scenario? I assume, probably wrongly, that as we are a manufacturer of them we may get first dibs on them.
up for anything wrote: » Are patients who are within some hours of inevitable death actually in any sort of condition to say goodbye to family via phone or iPad like I've heard they've been doing in Italy?
LadyMayBelle wrote: » Thank you so much for your advice and info, as well as your dedication. I'm glad you gave example of how you managed food delivery and wiping down items, as I worry about this as well as good intentioned people leaving items and bags of things at people's doors, esp elderly. I made clear in another thread that it's not about stopping kindness but a need to be mindful that more harm could be done than good? Once proper measures are in place then it's ok..ish. Would love your broken down list you referred to..we would have been chuckled at for being preppers but took a lot of advice from your posts. Thank you.
Funsterdelux wrote: » Howdy doody Pseudy, I was up on scaffold there starting to get the battens ready for slating the back of my cottage, the east wind is eating the face and hands off me. It got me thinking, with the measures of social distancing/isolation in place for months perhaps, other viruses such as the cold and flu would also find it hard to spread(i know we're going out of season). Would this have a positive or negative effect on our collective immune system? If a majority of us dont catch sars cov2 and other viruses, when/if things go back to normal would we be more at risk from getting a more severe cold/flu? The question always sounds better in my head, anyway thanks again and good luck!
trisha e wrote: » If suspected cases have to wait days for a test and,as a result, test negative because theyre better what is the point in testing if not testing for antibodies at the same time? Surely these tests should be allocated to people on the list with symptoms. A work colleague of mine was sick for 2 weeks GP booked a test on Monday and still waiting. Says he's feeling better now and wonders should he give his slot to someone else on the list. Thanks to you all.
fjortal wrote: » Hello and thank you so much for answering questions during this time. My dad found out he needs a triple Bypass a week and a half ago. He is meeting with the surgeon on Monday. He is 75 and will be tested for Cov 19. My question is, in your opinion, could I visit him in relative safety before and after the operation while keeping 6ft between us, wearing gloves and mask? I am in good health, no symptoms whatsoever. I do have children. I am extremely close to my parents and other family members have visited, keeping their distance. I am torn between fear of passing something on and the negative mental health effects not seeing them is having. Many thanks Fjortal
Potentially wrote: » Firstly, thanks, no words could say it enough Secondly: I am a single Mum with 12yo. Ex wants to continue contact, he has just collected her and has gone off for the day. He has been working as a salesman to pharmacies and has continued his normal socialising routines, with his new partner (nurse who home-cares for newborns) and others home recently from abroad.... I have been really careful to keep social isolation but is all that down the drain now? My elderly parents and aunts rely on me; and if I get ill, there is no where for my child to go. Please advise.
Notsomindful wrote: » Thanks for all you are doing. My local testing centre is a drive through centre. I have been referred for testing awaiting appointment. Can I walk to test centre- as I dont have access to a car and dont want to risk spreading it to others unnecessarily like taxi drivers etc...
RobbingBandit wrote: » Thanks for taking the time to do this. I'm a diabetic I've just had my next couple of appointments postponed indefinitely I am currently dealing with several complications including foot and eye issues which require routine care and can turn nasty I am unable to contact anyone in the departments so far and really don't want to find myself going to a&e. In short what is happening to patients with ongoing chronic issues in this current climate is my question.
Airyfairy12 wrote: » Hi I just have a question about coronavirus symptoms. Do they come on suddenly like in the case of a flu were you all of a sudden feel unwell or do they come on gradually, do you feel like youre coming down with something for a day or two before symptoms become obvious? Are swollen lymph nodes in the neck common with coronavirus like they are with cold and flu? Thank you so much for taking the time to answer questions.
The One Doctor wrote: » Does the current low number of deaths from CoVid 19 in Ireland give you any cause for hope about this pandemic? Thank you for your stalwart work.
digzy wrote: » Hi I’m a dentist. Like most of my profession I’ve shut my practice due to safety issues. Unfortunately the chief dental officer made a statement that we’re to work as normal despite not having appropriate PPE. Her advice is plain wrong. I don’t want to be a super spreader ( because I don’t have PPE) , nor put my staff or our families health at risk by remaining open. However I also feel a duty of care to my patients. The hse needs to order all dental practices to shut down. We might save a tooth but loose a life!
Bidd wrote: » If you’ve had the vaccine for pneumonia would this protect you from pneumonia if you get Covid-19.
begbysback wrote: » Given that deaths can be kept at a minimum by early diagnosis and treatment, are you guys lobbying for this, or just waiting at the doors of hospitals for critical cases?
Notsomindful wrote: » Thanks for link. That's reassuring for all of us who dont have access to a car/dont drive and dont want to risk.infecting others.in taxis/ high risk themselves...according to the hse, we" may be tested at home". So we may not get tested at all. Woohoo.
leggo wrote: » Thanks for doing this OP, first thread I’ll check anytime I’m on now. I’ve noticed a change in your tone and attitude towards the public over the past few days (not saying it’s unwarranted btw). Do you find yourself overwhelmed already with the workload and job ahead or do you feel it’s more your own personal anxiety about what’s to come? I’m trying to gauge what of this is based on your actual day-to-day work/lived experience and what is (educated) worry. On a similar note how do you compare your own state of mind to that of the colleagues you’re working with on the front line: are you one of the few preaching concern or are the majority of frontline workers freaking out about the public too?
Nonoperational wrote: » From reading your posts I suspect I know what speciality you are in but I appreciate you don't want to answer that publicly. I am heavily involved in GIM and have already completed numerous covid shifts in ED and have seen nearly 100 patients ?COVID. May I ask, will you actually be seeing COVID patients during this and be involved in their management? I appreciate you not wanting to let people know your speciality but could you at least clarify if you are GIM/Surgery/Psych etc. A broad category. Just so people have some context. Thanks
ooter wrote: » apologies if this has already been asked. it's horrible hearing the figures of people who may die from this virus but especially the fact that healthcare workers in our hospitals will also die, are all healthcare workers at risk due to their high exposure or is it the same as the general public, older with underlying conditions?
con747 wrote: » Do you think the number of cases so far is an accurate number? Also, is there a shortage of testing kits as 2 members of my family have waited 6 days after being referred for testing due to symptoms and underlying conditions and are still waiting. Thanks for your time and effort in this thread.
Beagslife wrote: » Hi Pseudonym121, Thanks for doing this. It's very informative and thought provoking. Stay well. My questions is regarding suppressants (not sure if that is the right term) like cold and flu medications/remedies. I used to typically get a couple chest infections (with harsh chesty cough and perhaps sore throat and sometimes fever) a year. For the last few years I find that at the onset of symptoms if I take echinacea capsules regularly I can usually hold it at bay and after a few days I am back to normal. Where I have let it get deeper I would add astragalus to help clear it up. By the way, I'm not advocating the above in any way, shape or form as regards Covid-19. Could the use of any of the above remedies by the general public cause problems by perhaps masking the Virus (reducing the symptoms and as a result people not looking for testing or being less cautious)? I think I read somewhere that some products had been banned in China for this reason. Possible fake news of course but perhaps you have better knowledge of this. Would you have an opinion on this? Sorry if it's not really relevant. Anyway keep up the good fight and take care of yourself.
Fleetwoodmac wrote: » Is there any truth in WHO giving directives regarding taking zithromax and chloroquine as prophilacs for covid?
Happy4all wrote: » Thanks for doing this and two questions if you don't mind: 1. My daughter works in a pharmacy and I fear for her health from additional exposure and then surely that impacts on the household's effort of social isolation, being made somewhat null and void. Should we be taken any additional measures? 2. The UK only reported 7 deaths today. A long way short of the daily 100+ prediction. Is this from lack of true testing numbers or signs that things are not as bad as feared?