....... wrote: » This post has been deleted.
AIMS Ireland are aware of many cases in which heavily pregnant women have been threatened “with the guards coming to get them” if they don’t turn up for their scheduled induction. In fact a cohort of women reported such statements are regular commentary at antenatal classes at one particular hospital
Edward M wrote: » A clear majority for repeal and the 12 week limit according to this.https://www.irishtimes.com/news/politics/clear-majority-backs-abortion-on-request-up-to-12-weeks-poll-shows-1.3368816?mode=amp
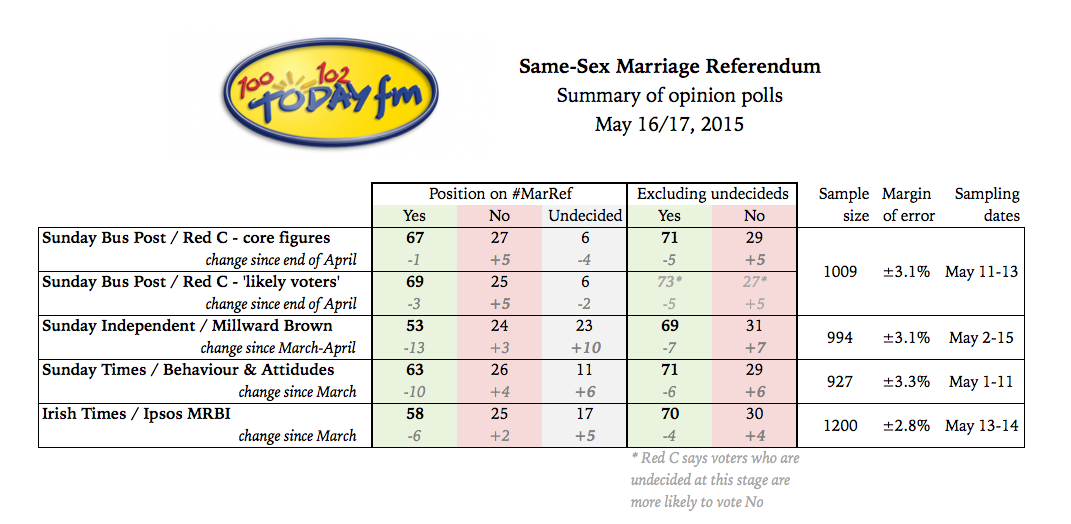
freshpopcorn wrote: » I'd be very concerned about the result of this opinion poll and I wouldn't call it a clear majority from my memory most of the opinion polls for the marriage referendum were well in the mid 60% and 70% and turned out to be about 62% and this could go either way being 56%.
New poll shows 76% support for same-sex marriage The details were in the first opinion poll of 2015.Jan 14th 2015, 9:45 PM
drkpower wrote: »
drkpower wrote: » http://www.thejournal.ie/opinion-poll-2015-same-sex-marriage-1882262-Jan2015/
drkpower wrote: » I'm not a fan of the 8th (far bloody from it!) but lets not overstate it. Before 1983, and after 1983, before the X case, and after the X case, abortions were being carried out in Ireland perfectly legally for many medical indications (for ectopics being the classical example). What the 8th (and the X case's interpretation) did was to legalise suicidality as a ground for abortion. Which is, eh, ironic to say the least! But irony aside, even now, and even post POLPA, i'm not even sure if an abortion has actually occurred under the suicidality ground (though may be wrong on that). So it might be a little misleading to suggest that the 8th did the complete opposite of what was intended.
seamus wrote: » "Official" means recorded, standard medical practice. I went looking (albeit not for hours) and could find no indication that abortion was standard medical practice in Ireland unless the embryo or foetus had no detectable heartbeat. And if abortion was standard medical practice when there was a risk to the life of the mother, what happened to Savita? Why was Malak Thawley refused chemical intervention and told surgical was the only option? Happy to be corrected though.
Joeytheparrot wrote: » Where there is a risk to the life of the Mother the hospital must wait until the risk is greater than 50% until they can act.
Loafing Oaf wrote: » Is this what happens in practice though? Surely we'd have a much higher maternal mortality rate if it was?
The number of maternal deaths in Ireland has risen sharply, and the pregnancy-related death rate is now higher than in the UK, according to a new report. There was a 22 per cent rise in the number of maternal deaths in 2010-2012, according to the second report of the Confidential Maternal Death Enquiry, based in UCC. The period coincided with a number of controversial deaths of pregnant women, most notably Savita Halappanavar in 2012.The rate of maternal death picked up by the report from hospitals and other sources is four times higher than official figures gathered by the Central Statistics Office from death certificates. The report, which says this issue is not unique to Ireland, recommends that a question on pregnancy status at time of death be added to the coroner’s death certificate. There were 38 maternal deaths between 2009 and 2012. Ten were classified as direct maternal deaths, ie due to obstetric causes. Twenty-one were indirect maternal deaths due to pre-existing conditions exacerbated by pregnancy. The rest were attributed to “coincidental causes”; these are not included when calculating the maternal mortality rate.
A girl deemed to be at risk of suicide who wanted an abortion was sectioned under the Mental Health Act because her treating psychiatrist said terminating the pregnancy “was not the solution”. The case is one of 22 reported by the Child Care Law Report Project, published this morning. In the case, which was before the courts last year, an order was made to detain the girl on the evidence of a psychiatrist who said that while the child was at risk of self-harm and suicide as a result of the pregnancy, “this could be managed by treatment and that termination of pregnancy was not the solution for all the child’s problems at this stage”.
Concerns have emerged at senior HSE levels about the failure to always secure a psychiatrist to give a second opinion in cases where a pregnant woman is seeking an abortion on the grounds she is suicidal. An internal document said in some cases it has meant the two psychiatrists and obstetrician, who are required under law to make an assessment in such cases, cannot be found. Abortion is allowed in cases of suicide risk under the Protection of Life During Pregnancy Act of 2013, which came into effect in 2014. The abortion can only be allowed if the doctors agree she is suicidal. If she is turned down, the woman then can apply for a review before another panel. However, in an internal report authorised by Dr Philip Crowley, HSE national director for quality improvement, the lack of availability of a "second opinion" psychiatrist at the initial assessment means that in some cases the woman's application is going straight to review. Some consultants "are referring to the review process before exhausting all opportunities to get the required second opinion locally", the document obtained by the 'Medical Independent' revealed. Objections
Bannasidhe wrote: » Similar to the difference between HSE 'on trolley figure' and the figure provided daily by the Nurses there is a discrepancy between the 'official' and the 'actual'https://www.irishtimes.com/news/health/new-report-reveals-sharp-rise-in-number-of-maternal-deaths-1.2111831 Firstly - do you really expect that there is a section on death reports that covers 'treatment delayed until risk of life to mother was over 50%' ? Secondly - Even one death is unacceptable when it could have been prevented by a termination of the pregnancy before things reached crises level. Added to that do we know how many suicides have occurred due to unwanted pregnancy? Pro-Life Psychiatrist Patricia Casey claims there have been none but as it is not recorded on a Death Certificate if a suicide victim was pregnant unless each post-mortem result was researched and the figure complied from that there is no way of knowing... We do know that those presented as suicidal are not always treated with sympathy and the system in place is not working - in addition to being a horrific ordeal to put a person in crises through in the first place.https://www.irishtimes.com/news/social-affairs/girl-sectioned-after-psychiatrist-ruled-out-abortion-1.3116111https://www.independent.ie/irish-news/health/suicidal-women-struggle-to-get-second-opinion-when-seeking-an-abortion-36532604.html
pitifulgod wrote: » Hmmm, posting random tweets that are pretty reasonable overall but outraged you, so you must tell the world. :P
Ralf and Florian wrote: » How stupid is this? It's the likes of this wan (Steph F) who will swing the undecided towards voting in favour of the 8th.https://twitter.com/Stephanenny/status/956885048044769280
Water John wrote: » Just to be clear, any sign of sepsis and medical will and should act, with medical intervention. Anything less is very poor practice, irrespective of the 8th.
Our investigation established that hospital guidance assumes four-hour monitoring of patient observations for patients with premature rupture of membranes. However, in this case monitoring of the patient who had prolonged rupture of membranes was less frequent (See Appendix F). There was inadequate assessment and monitoring that would have enabled the clinical team to recognise and respond to the signs that the patient’s condition was deteriorating due to infection, together with non adherence to guidelines for the prompt and effective management of sepsis, severe sepsis and septic shock when it was suspected or diagnosed. The modified Obstetric Early Warning Score (mOEWS) observation chart was not in use in some hospitals at the time of this incident for pregnant women on gynaecology wards. We considered that the patient’s condition involved prolonged rupture of membranes, which is associated with increasing risk of infection with the progress of time. In this case, the patient’s condition was rare and serious. There was a lack of recognition of the gravity of the situation and of the increasing risk to the mother which led to passive approaches and delays in aggressive treatment. This appears to have been either due to the way the law was interpreted in dealing with the case or the lack of appreciation of the increasing risk to the mother and the earlier need for delivery of the fetus. When the patient and her husband enquired about the possibility of having a termination, this was not offered or considered possible by the clinical team until the afternoon of the 24th of October due to their assessment of the legal context in which their clinical professional judgement was to be exercised.