Advertisement
If you have a new account but are having problems posting or verifying your account, please email us on hello@boards.ie for help. Thanks :)
Hello all! Please ensure that you are posting a new thread or question in the appropriate forum. The Feedback forum is overwhelmed with questions that are having to be moved elsewhere. If you need help to verify your account contact hello@boards.ie
Now ye're talking - to a consultant in the HSE [ANSWERS thread]
-
16-03-2020 9:43pm#1Boards.ie Community ManagerJoin Date:Posts: 10871
Answers from our AMA guest to questions asked in the Questions thread.
Please only post your questions in the dedicated thread here.10
Comments
-
Hi, I'm the HSE Consultant who is doing the AMA. I'm NOT representing the HSE, just trying to help out by providing some answers to questions people ask... I'm going to start by reserving a few posts which I intend to use to post some particularly pertinent information.
Then I'll start replying. I went asleep as soon as I got home and only just woke up so I'll be up for a while yet answering questions listening to my youtube playlist.
P.s. Please keep comments or questions in the questions thread. The main reason I agreed to do the AMA is that I want my answers to be available in one place for people to read without being buried in a swathe of comments, jokes etc. I'm trying to do this as a public service during this difficult time.0 -
I'm going to use this post to link to webpages/sites which I believe could be useful for those with medical questions/specific risk factors. I am willing to give some general opinions and repeat information which appears factual and has been published by reputable sources but specialist bodies and your own GPs and Specialists are definitely the place to go for individualised advice which will always be more useful to you as individuals than any general broad advice online. I am NOT offering anyone specific, individualised medical advice and wish to be clear on that. If you want that phone your GP or Specialist.
1. WHO myth busting page... VERY useful at this time. Some of the advice and rumours online are just so dangerous.
2. WHO Coronavirus page. Lots of useful, detailed, evidence based advice there.
3. HSE's Coronavirus page.
4. Royal College of Obs & Gobs UK advice re: Pregnancy & Coronavirus.
5. UK Asthma Society Coronavirus Advice
6. Irish Asthma Society Coronavirus Advice
Errata:
1. Phylogenetics of SARS-CoV2
2. COVID-19 Infected/Recovered etc Updates
3. A really good site for getting a breakdown by country, by date and multiple useful categories. Very succinct and easy to comprehend.
I'll add to this as0 -
I posted this previously in the mega thread but I think it is useful to repost it here for those who wish to learn how best to use masks, gloves, handwash etc. There's the normal way you do these things - which is effective - and then there's a medical way - which is likely to be MUCH more effective. If you've gone through the time and effort to do these things then you might as well get the greatest benefit possible from them.
Social Isolation:
Lets be very clear the best way to avoid catching SARS-CoV2 and avoid passing it on to other is Social Isolation. Social Isolation is far superior to any other strategy but it isn’t always feasible, especially if you’ve got a job which involves public interaction. With that said the safest thing you can do is socially isolate yourself as much as possible.
What does this mean? If you’re retired or otherwise not working at this time then stay at home. Don’t go out unless it is a matter of life and death – you must get food or you will starve or you must get medicines. Even in these cases I would ask why you have to go out? Have it delivered by the shop or pharmacy or have a relative who has to be out and about for work pick it up for you and drop it at your door without coming inside.
Social Distancing:
If you absolutely must go out to the shop then don’t touch others, don’t stand within 1 metre ( preferably two metres ) of them and don’t dally. Don’t lean against counters, don’t use cash, go contactless or if you absolutely must pay in cash let them keep the change or put it in the charity box. Don’t touch staff’s hands to get a few pence back and then put potentially infected money in your pocket contaminating your hands, clothes etc. Get in, do what needs doing and get out. SARS-CoV2 is very infections even with limited contact.
If you are working in a job where you cannot work from home then socially isolate as much as possible from other employees and members of the public. All of the above advice applies.
If you decide to go out for something non-essential then simply don’t. By doing that you risk catching and spreading SARS-CoV2. If you catch it and pass it to two people and they pass it to two others and the doubling rate is 4 days then after 28 days you will be responsible for 128 people having it. Of those 128 people 2 to 3 will die. Was that worth the price? I would argue that almost nothing except a matter of your own life and death or essential work warrants putting others at that risk.
Face Masks:
A lot of conflicting things have been said about face masks. The bottom line is that most of the face masks people are purchasing aren’t of any use and even if they were members of the public don’t know how to use them appropriately in order to gain effective protection.
For this reason I would say that buying face masks is ineffective UNLESS you have been advised on which ones to purchase and how to put them on, fit them and take them off. There is going to be a huge shortage of face masks for medical staff in Ireland soon. In Italy many hospitals have run out of face masks and the doctors and nurses have been treating patients without wearing facemasks themselves. This pretty much guarantees they will get infected and is why we’ve seen a rise in the number of doctors and nurses dying in Italy in recent days.
The only face masks which are worth getting are surgical masks or ones rated as either N95/FFP2 or N99/FFP3. Simply put these two ratings mean they stop 95 or 99% of particles above a certain size IF put on properly but almost certainly the vast majority of you with these masks aren’t getting any protection from them.
So, now that I’ve told you that in all the panic you’ve probably bought masks which won’t screen out viruses AND even if they did you don’t know how to wear them properly so as to protect yourself AND even if you get that bit right the way you put them on and off will spread infection do I offer any solutions? Sure, if you’ve already bought them you’re hardly going to return them to hospitals so the people who really need them ( front line healthcare workers ) can benefit from them so you might as well learn how to get some benefit from them.
Here are three good videos I have found and can recommend to show how to put on, fit and remove both surgical masks and more general oval N95 face masks.
How to properly put on, fit and remove Surgical Masks:
https://youtu.be/OABvzu9e-hw
https://www.youtube.com/watch?v=2xLjCfmx0iE
N95 Oval Type Mask:
https://www.youtube.com/watch?v=zoxpvDVo_NI
Once removed the face masks should be placed in a bin which is in a relatively well-ventilated area and which you don’t use often. I use a bin on a balcony which has no risk of being spread to others and also doesn’t act as a source of infection in the living area and has no risk of spreading to my neighbours.
Gloves:
Buying pairs of disposable gloves is a reasonable precaution. I, personally, have purchased several hundred pairs of vinyl, transparent powder-free gloves as they don’t irritate my skin as much as powdered or latex gloves. Why transparent? Well, they don’t attract as much attention when out in public. I’d also consider whitish ones. If you can’t source them then any colour will do. This isn’t after all, about fashion.
Again, gloves are almost useless if you don’t know how to use them properly. There is a set procedure for how to put them on and remove them and, yes, you guessed it there’s a video for that.
How to put on and take off surgical gloves without contaminating oneself.
Once removed the disposable gloves should be placed in a bin which is in a relatively well-ventilated area and which you don’t use often. I use a bin on a balcony which has no risk of being spread to others and also doesn’t act as a source of infection in the living area.
Do NOT re-use them. If you do that you might as well just go around shaking hands with everyone you meet and then smearing your hands all over your face repeatedly every few minutes.
The gloves won’t help much if you keep touching your face. The outside of the glove will transmit COVID-19 droplets to your face readily. So is there anything you can do to prevent yourself subconsciously touching your face out of habit? Yes, read the next paragraph.
Doctors and nurses need to get used to not contaminating sterile gloves by touching our faces or other non-sterile things. I’ve always found it useful to purposely interlace my fingers so that to touch my face I’d have to consciously uninterlace them. Since this isn’t always practical and with COVID-19 we are less worried about maintaining a perfectly sterile environment I’ve taken to carrying a tissue in one hand and a biro in the other. I find that carrying something in each hand prevents the vast majority of habitual face touching because I don’t want to poke my eye out with the biro and/or I have to move the tissue in order to free that hand up. By the time I’ve thought of doing that I realise what I’m about to do and can prevent myself from touching my own face. You might find different things that work for you, this is just something that works for me.
Handwashing:
Handwashing is a good idea but, obviously, social isolation is the best followed by social distancing and protective gear ( masks and gloves ). After all of those though it is still well worth washing one’s hands…. Yeah you’ve guess it…. So long as you do it properly. The sort of handwashing most people do verges on useless. On the positive side there are, as ever, videos to show you how. Here is one I found useful and have recommended to non-clinical staff/friends and family.
How to wash your hands the medical way.
As ever, I'm simply providing some basic advice and links to videos by reputable sources. If you don't like it, do it your way and take your chances with your own style of doing things. I'm just telling you how generations of doctors and nurses have been trained to do these sorts of things. If you think you know better then you do you.0 -
another post0
-
last one and then answers0
-
Advertisement
-
Thanks for the question. Honestly that would depend on what your underlying conditions are, the severity of symptoms you exhibit and your likely progression as well as what allergies you have so it is impossible to give a one size fits all answer here.What medicine should be taken if symptoms start to develop?
With that said the best advice is that IF you start having symptoms you should contact your GP and be assessed by them ( almost certainly over the phone ) and follow their advice. At this point in the pandemic in Ireland most people who think they have COVID-19 don’t, they have other more common viral or bacterial infections or even just psychosomatic issues. So long as you aren’t allergic I think you can’t go wrong with some paracetamol, rest and ensuring you are hydrated though.
As re: NSAIDs the best thing I can do is link to the HSE's advice. Might this change as we know more? Certainly but this is the advice as it stands at the moment. You'll have to make up your mind whose advice to follow. I have no reason, at this time, to doubt the HSE's advice on this issue.dartboardio wrote: »Hi,
Do you find yourself turning away lots of patients who don't have any real symptoms of the virus and are just taking up waiting rooms out of worry?
Are all your staff/colleagues full of panic/worry ? Is this the busiest you have ever been?
Thanks for the questions. I’ve certainly heard of a lot of people thinking that because they have a cough or whatever that they might have COVID-19 and I’ve heard a lot of frustration from people who want to be tested but don’t meet the criteria for testing.
It should be noted that Ireland had very few testing kits although that number is ramping up massively and will continue to ramp up. As availability increases the criteria for testing will be widened until we reach a point where we can test everyone we should be testing.
A lot of GPs are really struggling with the numbers of people phoning them seeking advice and testing and that isn’t helping. Thankfully most of those people have the sense not to come in in person and:
A) Clog up waiting rooms and") Risk spreading it to others if they do have COVID-19
Risk spreading it to others if they do have COVID-19
I don’t think patients are being turned away but there are a lot of worried well who would do best to just self-isolate, phone their GP and then follow the GP’s advice. On a population level you don’t need to do anything amazing, just follow governmental advice and your doctors’ advices.
My medical colleagues and I ( Consultants and NCHDs) are worried but not really about ourselves so much, although we do know that if this gets really bad then we ourselves and our friends and colleagues stand to have higher rates of infection and mortality per capita (age adjusted) than the rest of the population. This was seen in both swine flu and SARS and I expect it will be seen with SARS-CoV2/COVID-19 also. What I see and hear much more than that is a grim determination to do our duties and pay whatever price needs to be paid. I’ve been saying for a while now that we need to gear up as though Ireland is about to fight a medium-sized war, with all of the sacrifice and difficulty and loss that that entails. I’m starting to hear colleagues use the same language … I heard it said a few times today.
This is going to be a war, there are going to be losses but I think the vast majority of doctors are determined not to let Ireland down, no matter the cost. Sure we REALLY don’t want to die ourselves but we’ll do our bit, roll the die and know it’ll happen to some of us.
I, personally, am more worried about my parents than I am about myself and I think anyone with parents feels the same way. You have to remember we’re just like you in terms of families and being more concerned about those we love than we are about ourselves right now.
I’m not a spring chicken anymore and I have two underlying health conditions which increase my risk of dying if I catch COVID-19. I estimate I have a 15 to 20% chance of dying if I catch it but I’m going in because that is what is needed to try and save as many people as possible. I don’t think my place is directly on a COVID-19 ward because I’ll absolutely catch it for sure then and I won’t do anyone any good becoming another patient and using up resources which could be used to treat others but I have a role to play and I’ll play it. I think everyone else feels the same.
My nursing colleagues have the same attitudes really. I know nurses who have been doing non-front line duties for years and who have worried wives, husbands and children and have simply accepted that they’re going to be deployed wherever they can do most good. They know the risk this puts them at --- nurses also die at higher rates per capita ( age adjusted ) during pandemics --- but they’re not going to let you, the public, our patients down. Some, with health issues etc, will be deployed in places where they are less likely to catch it so that they can contribute care as opposed to consuming it but everyone’s grimly determined to do their absolute best.
As for allied health professionals… Well, the secretaries and admin staff are still showing up, doing their best as are the OTs, Physios, Dieticians, Radiographers etc… And let’s not forget the security staff, porters, kitchen staff and cleaning staff. A few weeks from now it will be a definite act of courage for a kitchen staff or cleaning staff to come into work because they’ll be exposing themselves to high risks of infection with COVID-19. Some will falter but I expect the vast majority to continue showing up and doing their bit. We need them ALL to do their bits because doctors and nurses on their own can’t make a hospital or GPs surgery run. It is a team effort.
I do think that some the allied health professionals who haven’t done nursing or medical duties on wards don’t quite “get” just how serious this is yet. I’ve definitely had push-back from some line managers about instructions I’ve given my team because I wasn’t following HSE protocol etc but this isn’t because they’re bad people or managers it is just because it is a big ask to go from peacetime HSE footing where there’s a protocol for everything and a change in work practices is a big deal to a mindset of, this is war and in war we do WHATEVER is necessary. When the whistle sounds, we all charge, we won’t all make it but we all charge. That is one hell of a mindset change and it takes time to make it… but even today people who hadn’t made the adjustment yesterday were contacting me to let me know they’d made the adjustment and were now of the “do whatever it takes mindset”.
A lot of (insert expletive of your choice here) ;-) is spoken about the HSE and, to be fair, some of it is even justified but, right now, while I’m a bit scared for myself and my family and I’m sad that some people I’ve known and worked with aren’t going to survive this it really makes me proud of Ireland and the HSE and socialised healthcare in general to see people knuckle down and prepare to go to war and fight this. We aren’t all coming back but we won’t let you down. We will, to quote the Marvel Universe, make the Big Play.
One thing I would just say on a slightly self-serving note is that when this is all over and a year or two from now doctor and nurses etc are advocating for funding and better working conditions please do remember who ran towards the fire at this time while everyone else was avoiding it as much as possible. Support us as much as we will support you in the months to come.
I’m sure this applies to the Army and Fire Brigade and Gardai and many others as well. I just don’t have as much contact with them so can’t address their attitudes directly.
Is this the busiest we’ve ever been?
No, a lot of the people who used to clog A&E with stuff that they should never have come in with seem to be staying at home. I don’t know if this is out of civic duty or fear of catching COVID-19 but myself and a lot of colleagues are ticking over doing the day jobs but aren’t as swamped as we usually are with the worried well etc.
We’re all still busy though as we’re preparing for what is to come.0 -
expectationlost wrote: »is it possible to protect yourself from the covid19 and treat patients, how are health workers still getting sick?, are not wearing some level protection now?
Thanks for the question. Well, you wear protective gear - goggles, masks, gloves, possibly even full coveralls over the other protective gear, taped up to prevent air flowing in or out. They're hellish to work in and exhaust you very quickly. This is one of the reasons you heard about Chinese healthcare workers dying of exhaustion and/or dehydration when they were battling this.
Why will health care workers still get sick? Cause viruses are tiny, we'll all be working long hours in exhausting stressful conditions and it only takes the tiniest mistake to get infected... especially when you're working in a ward or room in which the virus saturates everything because it is full of people with COVID-19 just spewing it into the air and on all of the surfaces as they breathe/move etc.
As to protective gear being worn now. Sure, in some areas, but we don't have limitless stocks of it and if we use it all now we won't have it when we really need it. If you listen to the reports from Lombardy in Italy doctors there are talking about running out of face masks and having to go into COVID-19 without facemasks ensuring they will catch it. Doctors and nurses and paramedics etc are dying there as we speak. Healthcare workers in Ireland will be dying in a few weeks time, alongside the members of the public they've been treating. There's no avoiding that now. We just need to knuckle down, do our best to protect ourselves and yourselves and pay whatever price we need to pay to try and save as many as we can.TheValeyard wrote: »Are there still the usual cough, colds, flu going around that could also be affecting people. If my toddler has a runny nose and slight cough, it's not immediately Covid19 but still the usual suspects?
Good question. Yeah, I right now have a runny nose and a dry cough but I've had that for a few weeks. I've had a tangential exposure to a COVID-19 patient last week and so I'm being careful about my contact with family etc just in case BUT even in my case since the cough etc predated the exposure this is almost certainly just the normal stuff that goes around this time of year rather than COVID-19.
The same applies to your and yours, except even more strongly. Right now if you have those symptoms you are far more likely to have something other than COVID-19. If the public doesn't play its part with social isolation and distancing, hand-washing etc then that may not be the case a couple of weeks from now.
With that said while children do seem to be able to be infected they do not seem to be at high risk of becoming severely unwell. So you can allay your concerns there somewhat. If in doubt though do keep your toddler away from elderly relatives. Just because the toddler won't become severely ill doesn't mean that whoever they pass it to won't die.I have so many questions, where to start as an asthma sufferer ( and nothing on line ) how do you differentiate between an asthma attack or Covid19?
as an asthma sufferer ( and nothing on line ) how do you differentiate between an asthma attack or Covid19?
Well, an acute asthma attack is acute and should be relieved by whatever inhalers your GP or respiratory specialist has prescribed while COVID-19 will come on, last over time and often be associated by symptoms other than shortness of breath.
That's just very general advice though.... If in doubt contact your GP and allow them to assess you and follow their individualised advice.Do you think that our effort to shift the curve and flatten growth will be successful?
Thanks for the question. I don't know, it ALL depends on what members of the public do. The scenes with people going out to pubs over the weekend made my heart and the hearts of my colleagues sink. Some of the people in those pubs will almost certainly have been infected and will have passed it on to other.
Superspreaders are a real thing with this virus and Patient 31 in South Korea appears to have infected over 1,000 people, roughly 1 in 8 of ALL cases in the country. The last thing we need in Ireland is someone like that. If they infect 1,000 people you can expect 20 or more to die.... and yet people were draped all over eachother in pubs. If Irish people continue to do this it will cause more infections, more people to become seriously ill and run a greater risk of overwhelming the health service and increasing the death rate from roughly 2% ( if we have enough ventilators ) to up to 10% ( if we run out of ventilators and capacity in the health service ). You are seeing this happen in italy where the % mortality rate is creeping ever upwards towards 10% as their health service becomes more and more overwhelmed.
We need to make that sort of behaviour as taboo as incest and child abuse for the duration. Otherwise it will condemn other Irish people to death over coming weeks and months.Or that we took our measures a week or 2 too late for maximum efficacy?
Well, the best time to plant an oak tree was 25 years ago. The second best time is today. I'm definitely of the opinion that we need to have the strictest possible measures today but, you have to bear in mind that this is an unprecedented situation for most governments and governments don't turn on a dime, they take a long time to change course. Given the realistic exingencies of governing a country I think the government is doing OK actually.
I think we've completely missed our chance to be Singapore but they had experience with SARS and learned a lot of lessons. One of those lessons was to go in hard and early if this ever happened again. They went too easy initially with SARS. I think European governments are going to have that same experience now but I don't think this makes them negligent or anything like that, it just means that it is really hard to change your mindset and get your head around how bad this could be and what measures are really needed.
For example, when I started posting about this a fortnight or more ago because I felt people weren't taking this seriously enough I was called a scaremongerer and a lunatic and was abused for posting. Now, much of what I said then appears really mild compared to what is actually happening and going to happen over the coming week and into the future.
So, yeah it would have been better to be stricter sooner but it takes people time to get their heads around this. At least the Irish government isn't taking the callous approach of the British government. We're still putting people first as much as possible0 -
CtevenSrowder wrote: »How long do you think the lockdowns will be required to last?
I don't think anyone knows precisely but any lockdown will need to last long enough to significantly impact on the chain of infection. To do that you MUST exceed at least one incubation period. Anything less than that is utterly useless. So that gives us a lower bound of 14 days. The more multiples of one incubation period you lock down for and the more completely the lockdown and social isolation is observed the better.
So, 8 weeks is better than 6 which is better than 4 which is better than 2.
I assume that what the government will do, and I have no behind the scenes insight into this and if I did I wouldn't be answering this question, is lock down for 2 to 4 weeks initially ( 1 to 2 incubation periods ) and then re-assess the situation. Then they'll decide whether they need another 2 to 4 weeks at the same intensity or whether we can ease it up a gradually.
How can you help at this time? Observe social isolation, handwashing, social distancing etc. The more strictly the public observes these measures the quicker the less transmission we will have, the fewer people will get sick and die and the quicker the lockdown will be over.
It is very true that while healthcare workers can save many of those who get sick it is you, the public, who can beat this. If you all go out and stand next to eachother in queues, don't wah your hands etc etc then the healthcare system WILL be overwhelmed and we will be traumatised as a nation like we were with the famine. If you follow all the advice about social isolation, distancing and handwashing and stay in as much as possible then this will hurt but we'll get through it fairly ok.CtevenSrowder wrote: »Why is it presumed that warm weather will reduce the number of cases?
Well, that's because a lot of respiratory viruses have a seasonal component and people are assuming that SARS-CoV2 will also. This seems to be a reasonable assumption but we don't know if it is correct. We could be surprised.
I think most people are using the Spanish Flu model where it hit in three waves, early 1918, October to December 1918 and then again in Spring 1919 before being pretty much burnt out by the end of 1919. Is that the right model to use? Well, it seems reasonable but we don't know for sure.
A reasonable question but not one I will not answer for the following reasons:sgthighway wrote: »What is your speciality?
1. when I posted here initially a few weeks ago I got abuse for posting. People online can be horrendous to eachother and I don't care to expose myself and my family to that abuse online or in the real world. If my identity became known I fear that could happen.
2. The HSE can be very vindictive and were I to identify myself I don't trust them not to go after me if I survive this.
I'm being careful not to present myself as an HSE representative. I'm just a doctor answering questions using my experience and knowledge to provide the best quality answers I can at this time of national emergency. I'm trying to be responsible in my answers and be open about the fact that I don't know everything and thus can't answer every question. Plus I'm fallible and make mistakes.
With that said when a Consultant came out a few years ago to talk about the trolley crisis the HSE went after him by querying whether or not he broke patient confidentiality in doing so. he clearly didn't but they just wanted to punish him and warn the rest of us to shut up. We're pulling together now but I'm very aware that if I survive the HSE management will likely return to their previous form and seek to punish doctors who say things they dislike - even if those things are true.
If I said what specialty I work in I would hugely narrow down the field for them to search to find me. I'm already concerned enough about Boards knowing my identity and technical means being used but:
a) I think this is my ethical obligation as a doctor and my moral obligation as a human
b) I think there's about a 15-20% chance I won't be alive in 6 months to be gone after and I'd hate to die thinking I hadn't done what I felt was right and
c) If I'm lucky enough to survive and they do decide to come after me then I'll just have to emigrate to Australia or Canada and get paid a lot more money for doing the same job. There are worse fates ;-)
So, I hope people will respect me desire to remain anonymous so as to avoid reprisals.History Queen wrote: »Have ye received any further guidance regarding coronavirus and pregnancy? Specifically the case in the UK where the newborn tested positive for the virus, has that changed anything regarding the treatment/guidance for dealing with pregnancy?
Thanks for the question. I think that the number of pregnant women who have been confirmed to have been infected is so low that it is difficult to draw any definitive conclusions. With that said I have been directing patients and staff ( there are lots of pregnant nurses and doctors who are worried about this on a personal level ) who are concerned about this to the Royal College of Obstetricians and Gynaecologists website which has a really good page on this:
https://www.rcog.org.uk/en/guidelines-research-services/guidelines/coronavirus-pregnancy/covid-19-virus-infection-and-pregnancy/
I think that explains it really well. I think the bottom line is that we must all assume pregnant women are more prone to infection and therefore they and their families need to be really strict about social isolation and distancing and hand washing measures.coastwatch wrote: »No question yet, but just to say a sincere Thank You to all HSE staff, frontline and support for the huge effort that has gone into the preparations for the spread of this virus, and for the ongoing effort that will be required to deal with it over the coming months.
Thanks. There has been a real sense of people beginning to understand the severity of this since the Taoiseach's statement last Thursday - which almost seems like weeks ago at this stage. Before Thursday some of patients and family members were complaining about delays in being seen or not being seen in person etc but today they seemed to understand that this was an emergency situation and previous norms no longer applied. Sure, not all of them but most of them ;-).
This is really helpful because over coming months a lot of assumptions about what the HSE should and shouldn't be doing are going to be thrown out the window. As a country but particularly in the HSE we're at war and we'll do our best for you but you need to understand that what you consider urgent and severe and what we consider urgent and severe is going to be very different over the next few months to a year. We're not trying to be unsympathetic but we're at war and we have a much better idea of what will keep most people alive at this instant. You'd better believe that's what we're going to focus on --- while doing our best to provide a service to everyone in the country who isn't infected with COVID-19.
For example: People will still get pregnant, get cancer, get asthma attacks, get heart attacks, develop depression, anxiety, OCD, have car crashes, fall and break bones etc. We are going to be dealing with ALL of the above PLUS COVID-19 and no-one suddenly found clones of us to flesh out the service. All we have to make up the numbers are redeployment of staff from non-essential services, retirees called back to the colours and early-graduation medical students and nursing students. With that said we will work harder than we've ever worked before (and we weren't slackers previously no matter what you might have heard or read) and will , inevitably, die in some numbers over the coming months but what we WON'T do is let you down. That simply isn't an option. We WILL be there for as many of you as possible for as long as you need us and as long as we can still stand.
I'm sorry if that comes across as wishy washy or emotional but, you know, I'm really inspired by my colleagues in the health service right now. Anyways, massive emotional outburst over for now ;-). My team would be surprised to think I wrote the above, this is another reason I can't be identified. I've got a reputation as a bit of a tough SOB to maintain and if I'm ever linked to this post my street cred with the cool kids will be totally shot ;-)
What you can do to help us is pretty simple but really powerful. You need to socially isolate, socially distance, hand wash and convince any of your friends and family who still think this is overblown that no, this is war and if they are selfish and think of themselves first and foremost they are going to condemn a lot of good people to death over the coming weeks and months.0 -
humberklog wrote: »Whenever my mate is asked what he does for a living he says "Doctor". He's an Ed. D (Dr. of Education) and does indeed work in this field (Adult education). Does it get your goat when you hear people claiming to be a doctor when their field is non med/psych?
LOL! That made me laugh. My dad has a PhD and always tells me he's a doctor too. I remind him that he's the useless type of doctor ;-) The greatest joy of my medical career is using the qualifications to harrass him ;-). Hey, I never said I was a good son, just his son ;-).
In all seriousness though, what your friend does for a living is work in education. And he worked really hard and needs to be commended for getting a Doctorate. That's quite an achievement and is to be respected but when one says one's a doctor I do think most people assume that means medical doctor so it does seem that he might be compensating for something --- hmm, I'm rubbish with the tech on Boards but this would, I believe, be the appropriate time to put in a winky emoji beside an eggplant emoji.
I'm happening and with it despite my age but the rest of you old foggies can have the coolest kid you know explain what I'm alluding to. ;-)Serious question. What would be your honest opinion of the current trolley watch numbers ? Why have they collapsed ? People didn't suddenly not require A&E or are the vast majority of A&E overblown ? Figures before Covid-19 over 300. Last year same time 180. This week reported as zero.
And thank you for putting yourselves in the way of harm to deal with this. It cannot be easy for your families.
Great question. When I worked A&E as part of my NCHD ( Non Consultant Hospital Doctor ) training scheme we used to get so many people presenting who didn't need to be there. It was cheaper or easier than seeing the GP. Or they were just drunk or high on drugs... I remember one guy who had been macheted 3 times by a drug dealer whose girlfriend he'd chatted up who kept physically assaulting us when we tried to help him. Eventually I gave the instructions to leave him be till he passed out from a combination of the drugs, drink and blood loss and then when he was unconscious we rushed him and were able to treat his injuries. A LOT of what presents to A&E should never have gone there and would be best dealt with by the GP etc. Every week I come across situations where someone has had an issue for 3 months or 6 months and done nothing about it but has now decided, at 2am on a Saturday morning that they need immediate review in A&E. It is ridiculous.
I think a lot of those kinds of presentations are down and I think that a lot of work has been done on the discharge/capacity side also. To be fair to the government the purse strings have been loosened and to be fair to management and the various Medical Colleges the rules and regulations which would hamper a response have also been set aside. Everyone has been freed up to focus on fighting the war instead of doing the paperwork.
As to families: Yeah, I think there's a lot of worry there alright... but we have to do what we have to do. It'll be far worse for everyone if we don't and by doing our jobs we don't just protect strangers, by doing our jobs and protecting those strangers we protect our loved ones also. I know that's in the minds of healthcare workers also. We are ALL in this together in a very real and impactful way.First off, sincere thanks and respect to you and all your colleagues for working at the coal face in these unprecedented times.
My brother is to be tested for covid19 shortly, I wouldn’t expect him to be in the severe risk category. I’ve read of non acute cases that develop ‘mild’ pneumonia. Can this category of patient recover at home without intervention?
Great question. I'm sorry to hear your brother will need testing. My thoughts are with him. The good news for him is that the majority of people who test positive for COVID-19 don't seem to require hospitalisation ( up to 80% of all confirmed cases ).
Of the other 20% it seems 10% need hospitalisation but don't need ventilation/high dependency care while 10% need ventilation/high dependency care. Deaths are overwhelmingly clustered in this latter group.
Obviously these are rough figures and they'll vary from country to country but the bottom line is that:
a) lots of people will catch it and have such mild symptoms they aren't even tested.
b) of those who are tested and are confirmed 80% won't need hospital.
I hope that helps allay some of your concerns for your brother.Boulevardier wrote: »A friend is having a small dinner party (4 in total) at her home tomorrow night. Is this contrary to current HSE advice?
BTW I don't understand where the answers are. I will try again.
Hi, here is a link to the answer thread:
https://www.boards.ie/vbulletin/showthread.php?p=112858492#post112858492
I asked Boards to preserve the answers thread for just answers as I wanted to have it be a concentrated source of reasonable, rational information. My hope is that people could direct family members and friends to it to have their questions answered. This is one way in which I hope to do my bit for the country at this time.
No it isn't contrary to current HSE advice and four people isn't a big high risk gathering. Still these sorts of "small" gatherings still increase the risk of passing it on above and beyond staying at home and self-isolating whenever possible.
My personal view is that when this is all over you can have all the dinner parties you want but right now I wouldn't be hosting or going to them. For however long this lasts the ONLY person entering my place is going to be the Tesco Delivery driver. I won't be having face to face contact with my parents, my siblings or my friends (outside of running into them at work). This isn't medical advice, simply me outlining where I'm drawing the social isolation line. The stricter we all are the fewer people will get sick and die and the sooner we'll be over the worst of this.Much respect and gratitude to all the doctors, nurses, ambulance personnel, in-hospital cleaners, admin staff, radiographers, porters, med lab scientists, etc etc.
All putting yourselves in the firing line, mentally and physically.
The vast majority of the public understands this....but you are more likely to hear from the terrified few who will shout at you.
Have you heard from your colleagues in Italy? and did the HSE start to ramp up capacity in line with the warnings that were coming from there last week?
Thanks for the kind words. As to the question... I haven't heard personally from colleagues in Italy but I'm well aware that in Lombardy they are reporting having run out of protective gear, treating patients without protection and growing numbers of doctors and nurses and others are getting sick and beginning to die. It is pretty grim but if they stick with the lockdown in about a month's time they should really see significant improvements and their situation could become more manageable. The death toll there is going to keep rising though. last week I calculated it was likely to exceed 1,000 a day before it starts to improve. Tough, tough days ahead for them.
I have a lot of friends in the US and they are beginning to get really terrified in medical circles. I think America is going to make Italy look like a walk in the park over the next year. Their federal government response is utterly incompetent and their healthcare system isn't set up for socialised care at all and in a pandemic like this having 10% of your population without any medical insurance or the infrastructure that a socialised healthcare system has is going to doom a lot of people. I think the states etc are beginning to realise this and take some action which will mitigate things but I'm really glad I don't live in America right now.
This evening one of my friends texted me that 20% of the doctors in their hospital are currently in self-isolation after exposure and they have ramped up the number of in-patients the interns can look after. They are supposed to limit it to 12 as a maximum. They are going to have to change that rule and god bless them but those interns and their patients aren't going to have good outcomes once they become overwhelmed.and did the HSE start to ramp up capacity in line with the warnings that were coming from there last week?
Well, I won't comment on specifics as I want to hold the line of giving advice but not divulging privileged information but I think it is fair to say that after the government was briefed last Monday a lot of people throughout the public services seem to have made preparing for this their number one priority. I don't know what was in the briefing to the government although I can guess because I ran the numbers for myself about 3 weeks ago and that's when I got scared and began contacting my family to inform them of what was coming and the need to prepare.... and then later decided I needed to try to raise the alert here because it didn't seem most people understood what was about to happen.
Anyways, I don't know what was in the briefing but I think it scared them sh**less and afterwards the government realised it needed to prepare for war.... and to the credit of the state all of the arms of the state involved in responding to emergencies ( Gardai, Army, HSE, Fire Brigade etc ) do seem to have taken this to heart and began preparing to go to war.
Massive efforts are underway to free up hospital beds and create extempore hospital beds throughout the state. I expect that those measures will be announced over coming days - I had thought they might start being announced Monday but I was wrong.Boulevardier wrote: »Not sure what is going on here. I have been several times now on the "answers thread" and there is nothing there.
Mea culpa, Mea Maxima Culpa ;-)... I was up till 3am working last night and so went straight to bed when I got home. I woke at half eleven and then began replying here. I think my hours going forward are going to be best described as "erratic". I'll reply as and when I can and do my best to address every question but, I hope you'll all understand that when this really gets going I may have to priotise things other than an internet forum.
With that said I personally think this could be a very valuable service and so I intend to continue replying here. If and when I get COVID-19 I also intend to post here with my obs ( temperature, pulse oximeter readings ) and other observations for as long as I'm physically able to because I think that might prove valulable. Don't know how but there's a long tradition of doctors documenting their illnesses which has proven useful later so I might as well do that in between bingeing Netflix ;-) I definitely need to crack out the Babylon 5 boxset again...begbysback wrote: »Is vitamin D really any good as a prevention of the virus, niacin in particular.
Niacin is Vitamin B3 not Vitamin D. I am not aware of any evidence that Vitamin B or B3 in particular is useful. By FAR the most useful thing anyone can do is to socially isolate, socially distance and hand wash. All the vitamins and other medicines in the world won't be as effective as simply not getting infected in the first place. I know that is really obvious but it does bear stating again and again and again.
I've heard of people saying that Vitamin D3 ( which is what I think you may have been thinking of ) may be beneficial in preventing cytokine storms etc and that Vitamin C boosts the immune system etc but I think we need to be really clear that the BEST thing anyone can do is socially isolate, socially distance and hand wash. If you sit in a room with an infected person who coughs and splutters and then touch surfaces they have touched and don't handwash then all of the Vitamins in the world won't help you.
With that said as I've gotten older I decided a couple of years ago to start taking some Vitamins which I felt had an evidence base for general health. I take a daily multivitamin containing cod liver oil and I take daily Vitamin C. Over the past two winters I have definitely had fewer chest infections than previously. I think part of that is that I also wasn't overworking myself as much and was trying to be a little bit more conscious of my stress levels but some part was probably the vitamins so I keep buying them and taking them daily.
Do I believe that Multivitamin and Vitamin C will protect me from SARS-CoV2? Absolutely not. Social isolation, social withdrawal, gloves and handwashing will protect me. Multivitamins and Vitamin C won't protect me if I don't observe the above precautions.
To put it another way multivitamins are great but if I were to smoke 40 cigarettes a day for 30 years I'd expect to get COAD and lung cancer no matter what vitamins I took. I hope that helps. Vitamins may be helpful in general but they are not the panacea some make them out to be.0 -
little bess wrote: »The Uk are asking over 70’s to self isolate, would you recommend the same thing to that age group here?
Yes, absolutely. My parents are in that age group and they've been self-isolating for almost two weeks now on my advice. They told me they went out to the pharmacy for medicines and I almost lost it with them... but they'd have been upset if I said that so I bit my tongue... They should have let me go to the pharmacy instead and take that risk instead of them.
So, I would advise anyone over 70 to really strictly self-isolate and have food and medicines delivered to them. Show them how to use kindle and netflix and let them spend the time reading, doing netflix and chill and skyping with everyone in the family. I've spoken with my family on the phone more in the last two weeks than I did all last year.little bess wrote: »I’ve heard diabetes, hypertension, copd are all extra risk factors, should these people take more care with social distancing?
Many Thanks
Yes, absolutely. It is unclear precisely how much these increase the risk of mortality but it is clear that they increase it. Most figures I've seen say each of these factors increases the risk of mortality by roughly 5% and having more than 1 of these risk factors would likely increase your risk of mortality more then 10% ( risk factors don't cause risk to go up additively they compound ).Gloomtastic! wrote: »What’s the difference between a bad dose of the flu and Covid-19?
Wow!!! I'm going to rephrase this question slightly so we are comparing apples to apples. What's the difference between a bad dose of the fly and a bad dose of COVID-19... Well the difference for people over 70 is the difference between having a 1 in a thousand chance of dying and a roughly 10% chance of dying. Those are rough figures but the general gist is that if you are over 70 you are 100 times more likely to die if infected with COVID-19 than the flu.
That SHOULD terrify anyone who has a loved one in that age group and why we all need to encourage them to socially isolate, get their messages, medicines etc and practice social isolation, social distancing and hand washing ourselves.
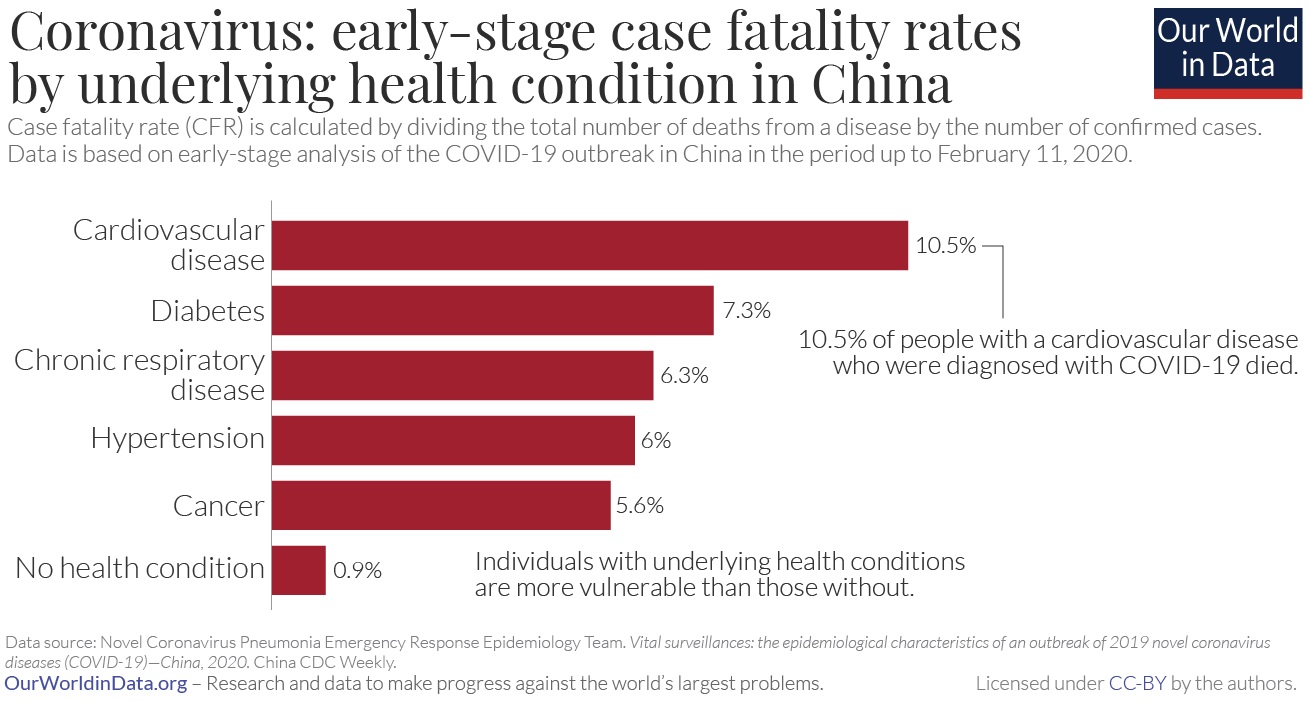
And lastly two pictures showing fatality rate by age and risk factor in China. It isn't the most up to date but I think they make the point graphically and eloquently.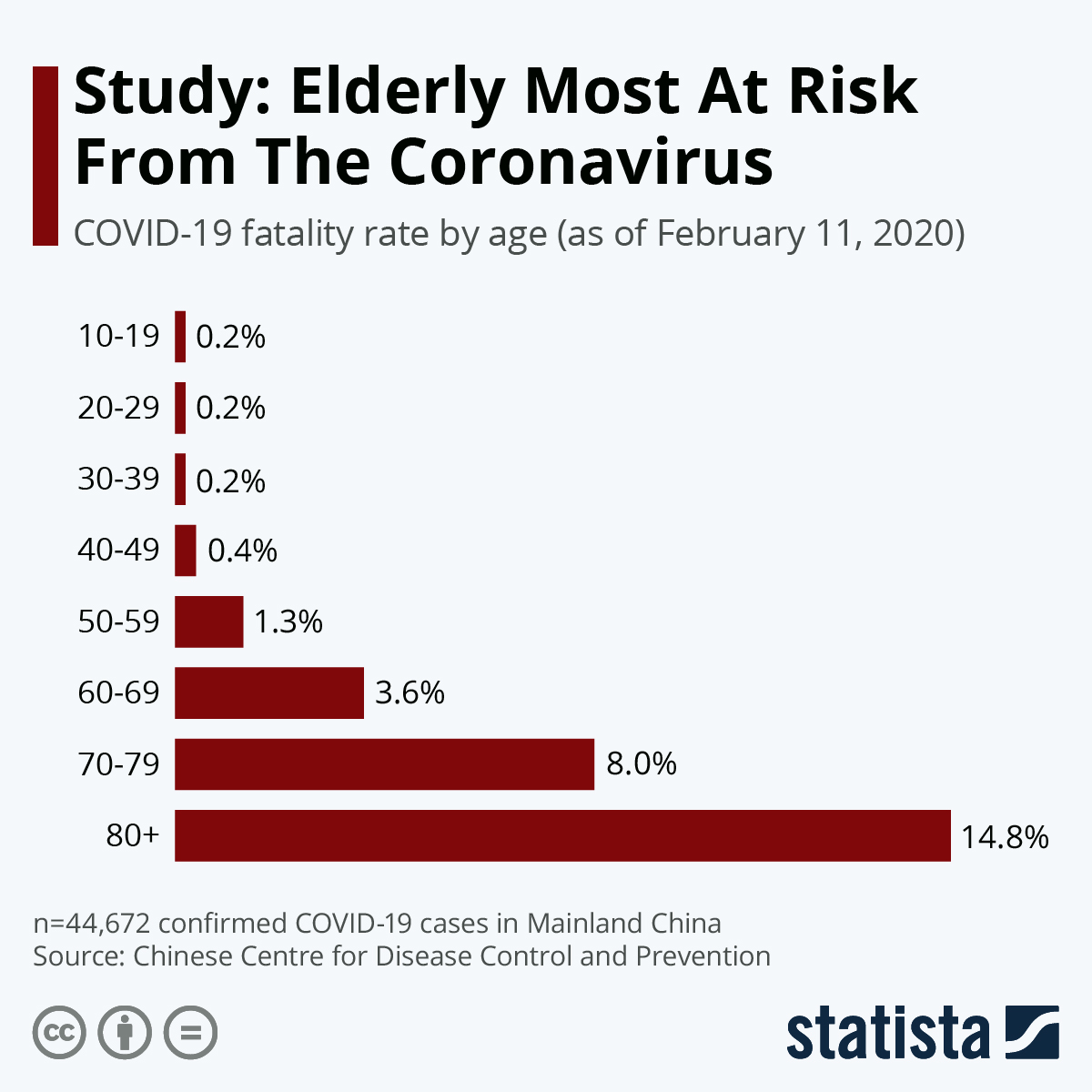
 0
0 -
Advertisement
-
patsy_mccabe wrote: »If someone gets the virus, get sick and get well again, at what point can they be confident that they have stopped shedding the virus?
This is actually a really interesting and important question, thanks for asking it. As with a lot of medical questions it has multiple answers depending on the level of certainty and detail of the explanation required.
E.g I can be asked the same question by seven groups of people generally speaking:
a) patients
b) non-nurses, non-doctors but working within the HSE
c) nurses
d) NCHDs
e) Consultant Colleagues not in my specialty
f) Consultant Colleagues in my specialty
g) family and non-medical friends
Each of them will require a different answer pitched at a different level because they come to the answer with different levels of knowledge, different anxieties and agendas and my role with each of them is different.
With a patient I might answer a question about risk factors for COVID-19 by saying:
"Well, here's two graphs which show you that the older you get the more at risk of dying you are and the more chronic illnesses you have the more at risk of dying you are. Now, in your specific case you are x years old and have y so that means your risk could be about z%. My advice on how best to deal with this is a, b, c etc."
With a junior doctor on my team this is a teachable moment and I would present that data, I would seek to personalise it for them ( which aids their learning and memory ) by relating it to patients they have recently seen in clinical - ideally patients I know they have formed an attachment with so that I can link an emotional response to the information and hopefully aid its remembrance I'd also talk about how this related to other illnesses they are more familiar with so as to help them contextualise this knowledge and then I'd invite questions and allow for discussion. I'd also be aware that this sort of question might be their way of asking about their own family members' risks and I would probably reference my own risk factors and estimated mortality if/when I am infected and then link that to someone in their family they'd mentioned previously and what risk factors they might have ( a pregnant sibling or spouse, parent etc). By doing this I'd hope to subtly give them permission to raise their concerns and ask what was on their mind.
I've done that with a few NCHDs in the last couple of weeks.
With Consultant colleagues the discussion might be as simple as:
"Oh you know, elderly and crocs."
With all the shared experience and argot and the ruthless training in efficient effective professional communication which is such a large part of our training we can communicate an awful lot with very little.
And yeah I do accept that doctors can be woeful when communicating with the public. ;-). I'm talking about efficient effective professional communication with eachother.
Anyways this is my way of explaining why I can't give you a nice simple answer. It seems that you can still shed the virus in faeces for quite some time even after you've gotten "better" but the real question we're interested in is not duration of viral shedding it is duration of infectivity.
You can still be shedding via faeces but this doesn't seem to have be a significant source of infecting others even though viable virus has been found in faeces.
In terms of sputum and droplets after getting "better". We don't know precisely. We are still learning. I think our current best guess is that if you're coughing you're definitely infective but once your symptoms have disappeared your risk of infecting others should be low. How low? We don't know yet.
Welcome to real world medicine. It isn't like on TV, in the real world there are lots of unknowns and maybes and "we think that"s. Plus people do really weird stuff writers would never even imagine putting in their shows.To re-word it, how are you managing to get time to do a Q+A on here? Has your actual working day/week changed with the virus? Or are ye folks still working the same hours, albeit arguably with more to do during those hours? Or has the trolley crisis suddenly getting solved actually meant that your working day is easier than it was before the virus became so known?
Good question. I've rambled on about it below... ;-)Has your actual working day/week changed with the virus? Or are ye folks still working the same hours, albeit arguably with more to do during those hours?
Same hours or more. I think we're just prepping for this to really hit and every extra day of preparation you all can buy us through social isolation, distancing and handwashing will help reduce mortality. Please buy us those days. Not for our sakes, but for yours and those you love in the risk groups.Or has the trolley crisis suddenly getting solved actually meant that your working day is easier than it was before the virus became so known?
Oh Jesus, I'd trade the trolley crisis for this any day of the week. Any doctor I know would be down on their knees giving thanks to go back to the bad old days of a trolley crisis without COVID-19 on our radars. Give me a thousand letters of complaint about waiting lists or how my NCHD said something in a way which made someone feel they insinuated x or y instead of this.... and I HATE those letters. I could be seeing patients cutting down waiting lists instead of writing replies to them.
What are healthcare staff doing with all of our free time these days? Girding our loins and preparing to go to war.
I'll tell you some of my preparations to give you a sense of it...
I ordered food delivers, disposable gloves, masks and various other protective supplies about two weeks ago. Enough to see me through about a month of food and 3 months of personal protection.
I got my family up to speed and got them to make the same preparations. I made sure my parents got 3 months of their medicines in so they wouldn't have to go out if/when this got bad.
I figured out what my mortality rate was and wrote a will for the first time. That was a surreal experience.
I made sure my finances are in order so that if I become ill, incapacitated and die they can be dealt with by my family.
I live alone so set up a plan of daily phone checks if/when I become infected so that should I rapidly deteriorate and become incapacitated or die an ambulance can be called to bring me to hospital or the morgue.
I don't expect there to be much point to my being brought to hospital though if things get really bad because with two underlying health conditions I wouldn't be intubated in Italy today so if it gets really bad here I wouldn't expect to be intubated. That's pity for me personally but terms the breaks. With that said I'm hoping for a good outcome here. 20% mortality means 80% chance of living so the world had better get ready for Party Consultant if I get out the other side of this ;-).
I've written letters to those I care for to open if I die.
I've packed certain things into boxes and labelled them with the names of whom I wish them to go to if I die and put them in the spare room along with written instructions.
I've packed non-essentials away so that:
a) I will have less clutter to deal with and
b) it'll make it easier to manage things for my family if I pass.
I had a think about what I would do once this was spreading in the community. I decided that I wouldn't go out except for work and food/medicines. I feel, as do my colleagues, that I/we have an obligation to the public to protect ourselves so we are available to treat them if/when they become ill. That means being a hermit for the next few months.
Then I had to decide what I would do with my time. There are a couple of shows I'd really like to finish to see how they end and Westworld Season 3 is starting so, you know, a reason to live ;-).
I then decided that with the rest of my time I'd like to be of use and try to help out. Posting to Boards.ie seemed like a pretty good way of doing that without having to go out #introversionforthewin ;-)
Professionally I've changed the entire way my team works, I've been trying to help management prepare any way I can, I've been talking to other colleagues trying to find any way I can to help them - and they've done the same for me - and I've reached out to other services and hospitals to see if there's anything I can do to support them.
Tomorrow I'll be splitting my time between dropping some stuff over to my parents, answering on boards and researching online, reading some HSE and NHS protocols, reading some relevant research and writing some proposals/procedures etc which might help another service. I'll also prepare food, clothes etc so I won't have to do anything but go to work and sleep for Wednesday to Friday.
It is all about prioritisation and time management. You don't become a Consultant without being able to ruthlessly prioritise and time manage. So, that's what I'm doing in order to prioritise the stuff I think I can be most helpful doing... and as you can see I've also thought a lot about my own mortality and the fact that I may not be here 3 or 6 months from now.
And, you know, nerding out watching Picard when it comes out... Mostly though I need to survive in order to see Season 2 of The Mandalorian #lifegoals ;-)0 -
All my Chinese students families have been wearing masks at home at all times. They take the masks off for bed. The children ( my students) do not wear masks. They have emphatically told me over and over again to wear a mask, at all times. That this is the success against the virus. I have been seeing my parents with masks on now for five weeks. At home.
I am wondering why the advice here is not to wear masks. is it that it is a false sense of security?
My chinese families do not understand why everyone here in the west is not being told to wear a mask.
Thanks,
Great question. To be honest I think masks for the public are worse than useless for one simple reason: People don't know how to put the masks on properly, fit them properly and take them off properly and therefore they are useless for most people.
Also, it is FAR safer to stay at home socially isolated than be out and about wearing a mask so I think the government has hit on one simple message and are focusing on that - socially isolate/distance and handwash. I think they are probably right to do so.
Almost every picture I've seen online of people wearing masks shows them not being worn properly and being useless.
Even with this simple message they are having to fight idiots who just make up lies and rumours which will kill people. If they went for more nuanced messaging it would be difficult to get a consistent message through to people.
With that said it is different for healthcare workers and people who know how to use the masks and MUST be out and about. E.g. I plan to wear masks on my way into work and home starting Wednesday. But I know how to put them on, fit them and take them off so they'll be effective for me, hopefully.
In the picture below from the BBC this mask isn't being worn properly and thus provides almost no protection. All this woman is doing is preventing a healthcare worker from using this mask properly and being protected at work. 0
0 -
PaybackPayroll wrote: »1. Do a proportion of people who recover have permanent lung damage?
1. Well, interstitial lung disease often results in long-term chronic lung issues with decreased long-term survival. We don't know what the long-term effects of COVID-19 infection will be but it is a reasonable assumption that a portion of those who have severe or moderate illness and survive will have long-term sequelae which will both limit their ability to function as freely as they'd wish and their long-term survival.
2. SARS-CoV2 hasn't been around long enough to say this for certain but I suspect we'll have to see a significant investment in respiratory clinics etc going forward.PaybackPayroll wrote: »2. Is the Irish strategy to get 60% of people infected and recovered, but at a steady rate so a not to overwhelm the HSE, or is there some other strategy?
No, absolutely not. The Irish strategy is to save as many lives as possible no matter what the cost. This is war and while this means people will die and Consultants are going to have to make horrifying decisions which will stain their souls and minds forever we are NOT going to write anyone off at this stage.
WE want to save EVERYONE we can so do your part and help us, socially isolate yourselves, socially distance and handwash. That's what you can do to save lives so please for the love of all that's holy do that and correct any muppet you see not doing it.
I'm not sure I understand what you mean by this. Could you clarify please, sorry if I'm being dense.PaybackPayroll wrote: »3. Roughly, how long does each phase of the illness last?PaybackPayroll wrote: »4. What is the current ICU capacity, and is this being massively ramped up?
Well, as a matter of public record we have about 250 ventilators in ICUs/high dependency beds. We also have additional ventilators as spares for when one goes down, ventilators in Operating Rooms etc. They are ALL being repurposed to front-line use.
Operating rooms (ORs) will become extempore isolation rooms - they're pretty good for this purpose actually but it will mean routine operations being cancelled. That's just a price we'll have to bear.
Private hospitals have more ventilators, probably mostly in their ORs and they'll all be requisitioned going forward. If you assume that someone who is amongst the 10% with COVID-19 who is most severely ill will need ventilation for 2 weeks to recover sufficiently to move onto supplementary oxygen every ventilator we find could save 24 lives over the next year.
So, holding a ventilator back will be tantamount to mass murder. We'll still need a few for emergency surgery etc obviously but every one not reserved for that purpose will need to be used to ventilate COVID-19 patients.
To give you a sense of what I mean by decisions staining souls lets do some mental maths here.
You're a surgeon in a hospital and you have to figure out how many ORs you can convert to COVID-19 patients. Lets say you have 8 ORs. If you convert 7 you can maybe save 168 ventilated patients a year... but if you have more than 1 emergency needing surgery at a time during that year the 2nd emergency might die before you can operate on them.
So you only convert 6 rooms... At the end of the year you find you only needed that 2nd OR 12 times... Sure, you saved those 12 lives at the cost of 24 others.
You did your maths in good faith but because you miscalculated more people died than needed to. You know this but tomorrow you have to go in and do it all again because your patients need you and if you break even more will die.
This sort of thing is what my Consultant colleagues are looking at right now. If we guess wrong now more will die than need to and we will carry that with us, always.
That's why I think we're going to have a lot of doctors quit medicine, develop addictions or commit suicide after this is over. I'm sure this will happen to other healthcare professionals also but when push comes to shove the Consultants and the NCHDs are the ones making these calls and the group I'm most familiar with obviously. Fortunately Consultants are tough... I think it is going to hit the junior doctors really hard. I'm worried about them, and the younger nurses too.
Anyways this is why I think we'll need to provide ring-fenced mental health care for healthcare workers after this. I think we owe it to them, especially the younger ones who haven't had time to develop the defences us old foggies have ;-).PaybackPayroll wrote: »Thank you for taking the time to do this AMA, and also for all of your efforts in tackling this horror.
Thanks. Others are doing far more but I hope this thread increases my contribution a bit. I wish I could do more.0 -
And that's me done for the evening/morning. I wanted to answer the first two pages. I'm going to bed now, catch you all later today. I hope you found some useful information here and you got an insight into how Consultants' minds work. We're... different.
") 0
0 -
Is this rumour true, that anti-inflammatories like aspirin and Nurofen make you more prone to the virus?
No, at this stage I've got Ibuprofen and Paracetamol and intend to use both if and when the time comes.
Official HSE advice and information about this issue can be found here:
https://www.hse.ie/eng/services/news/media/pressrel/advice-about-anti-inflammatory-medication-and-covid-19.html
The French Health Minister did come out with a statement advising differently but they appear to be in a minority of one in terms of countries and I expect that they'll change tack once more information comes in.
With that said asthmatics and others who may have issues with NSAIDs ( non-steroidal anti-inflammatories ) should exercise caution and follow their GP's or Consultant's advice regarding any medication to be taken if they are diagnosed with COVID-19.Just seen this pic online. Does it frustrate you that people are making up stuff and posting on social media?
Frustration isn't the word. This is willful sabotage of health on a national and global scale. Because people are scared they will panic and believe this sort of thing and it will lead to additional deaths.
When this is over I would be in favour of anyone who originates these sorts of things being charged with whatever the civilian equivalent of war crimes is.Scot_in_Dublin wrote: »Not a question, just a very sincere thank you to you and all of your colleagues globally who are working around the clock to keep the rest of us going.
Thanks. I'm trying to do my small part. Others are risking far more and doing far more in many places around the world.... the healthcare staff in Italy in particular are going through hell right now.Can you explain the 15 minute in contact time?
I think they had to come up with guidance early on in this. I think that at the time it was based on best evidence and useful because some people seem to assume that if you walk past someone with the virus then you're immediately infected. That isn't true.
With that said I don't think that sitting within 1 metre of someone who has COVID-19 for 10 minutes is somehow perfectly safe. Medicine and advice to the public needs to have certain cut-offs to make it easily understandable and you only have to look at the behaviour of some in our society to see that even very simple messages don't get through to some people.
So they went with the 15 minute advice which is a reasonable guide BUT I have always advised that social isolation or extreme distancing ( teleconference whenever possible, staying more than 2 metres others ) is far preferable.
Also a 2 metre distance won't do you any good if you don't handwash/wear gloves and touch something that has COVID-19 droplets on it and then touch your face.Ladybird18 wrote: »My child who is asthmatic is complaining with sore throat and nausea tonight.
Should I be worried?
That's an impossible question based on many factors including your baseline anxiety levels. What I can say is that children get sore throats and nausea from time to time. Nausea isn't a major symptom of COVID-19 and it is FAR more likely your child just has something other than COVID-19... remember all the other stuff that happens this time of year is still circulating in the community also.
In addition the death rate among under 18s is extraordinarily low. They can catch it and transmit it but they tend not to become too unwell themselves.
I'm linking a graphic I have recommended to a number of people when asked similar --- I have x is it COVID-19? type questions.0 -
What happens after you've self isolated for the 14 days after testing positive?
Have you built up an immuninty?
Could you catch it again?
And a big well done to all in emergency services and the HSE.
Well, if you test positive it isn't about waiting 14 days and then going out and about again. It is about waiting until you are symptom free, fully recovered + a few days. You will be advised about this by your GP or Consultant/treating medical team. That may be 14 days, it may be significantly longer.
Illnesses and human bodies don't run to schedules, when we have a lot of experience with them we can talk about the range within which most people fall but it is still early days with this virus and we are learning more about it all the time.Have you built up an immuninty? Could you catch it again?
You'll have built up an immunity to the strain of COVID-19 you caught. There is some evidence there might be another strain out there already although that isn't confirmed yet. The two strains are tentatively labelled L and R
What we do know is that RNA - which is what this virus is made from - has a really poor error checker and so mutations are very common. When enough mutations happen a new strain can develop which is sufficiently different from previous strains that having been infected by other strains doesn't confer immunity.
This is what happens with the flu and cold etc so that catching it once doesn't make you immune to other strains the next year, or even the same year.
Most doctors expect that SARS-CoV2 will mutate sufficiently to create new strains eventually, if it hasn't already, and thus become seasonal. When will this happen? No-one knows for sure.
I'll link to a really nice website which helps people visualise the phylogenetics of this. If you press the play button on the image on the right you can see the genetic drift as we've tracked it over time.
https://nextstrain.org/ncov0 -
LuckyLloyd wrote: »Best of luck over the coming days, weeks and months.
Are the HSE trying experimental treatments ala South Korea and China? I'm referencing chloroquine here and some of the old HIV drugs that have been mentioned.
Irish doctors will try everything they think will work. We've already got data from China and Italy and the US about some treatments which might work - retrovirals and monoclonal antibodies and suchlike. Doctors in every country are throwing everything at this and when we find things which definitely work their production will be ramped up like you can't even believe right now... any company which tries to make a signficiant profit out of any drug which will work will find itself destroyed by governments worldwide so I think that once we prove one or several treatments work they'll be produced worldwide in huge numbers. That will, however, take time. You've got to build the factory or repurpose the pharma site to produce this drug and that doesn't happen quickly or cheaply.
So, again, socially distance, socially isolate, handwash and do all of the things we need you to do to buy us time. We need everything but what we need more than anything is for the rate of infection to slow, lowering the peak, and time to build and buy ventilators, to convert hotels, barracks etc to hospitals and to produce more medical equipment ( in Italy they ran out of valves for their respirators and people are 3D printing them at home and rushing them to hospitals). People in Italy have died because the 50,000 Euro ventilator didn't have a 1 Euro part.
This leads me to another point...
Could people in the know here point me in the direction of ( or point others in the direction of me ) groups of individuals with 3D printers? Enthusiast groups and suchlike.
I think it might be a useful to gather a list of people with 3D printers and design ability who would be willing to help out by printing parts which could be used when/if current stocks run out in the hospitals. PM me with info please. The government may already be doing this behind the scenes but I haven't heard a peep and so I thought it might be good to put a call out here.
Hopefully we won't need this capacity but it is best to plan ahead now and then, if it is needed a month from now, it could be ready to go instead of only trying to organise it then. This is a time for lateral thinking --- and government departments tend not to be good at that sort of thing.I work in the public service as a Clerical Officer and there are rumours that we will be sent home on Friday. Is there any way I can volunteer to help out?
I don't know the official answer to that but I would suggest just letting your line manager know that if sent home you'd like to help out anyway you can. I think that, in the future, there will be lots of opportunities to help out with contact tracing or grocery deliveries to the elderly etc ( that mightn't seem like a big deal but it will free Gardai and Army personnel for more essential tasks and every bit helps).Can I ask if it’s true that “mile symptoms” can actually be like a nasty pneumonia, so while it’s medically mild it could really knock people back?
Yes, something we keep from you most of the time is that when you think you're severely ill we think, "Jesus, you haven't seen severely ill yet mate." We obviously don't say that because it wouldn't go down well and if you're feeling unwell it is severe for you and we get that.
Here's a rough guide i published previously... What most of you call severe illness is, at best, moderate to a doctor. Often it is mild. When doctors are talking about COVID-19 cases as mild, moderate and severe here’s what they really mean:
1. Mild: Doesn’t need hospitalisation. You may feel really sick, you may need home nebulisers, you may be on antibiotics. Doesn’t matter, if you don’t need hospital then you’re mild. Generally when people say they’re severely ill at home we don’t contradict them (since they certainly feel very ill) but in our minds you’re all mildly ill with varying levels of whining ;-). Doctors and nurses’ families will tell you how little sympathy they get from us when they tell us they’re sick. We’re the epitome of “If you aren’t hospitalised then you’re fine” even in general life most of the time ;-).
2. Moderate: One of the 10% who are hospitalised but don’t need ventilators. Some of those might still die but most will be just fine – albeit the interstitial lung disease may cause them problems in the medium to long term.
3. Severe: One of the 10% who need ventilation.
So, being "mildly" ill with COVID-19 could still really sick and take a month to recover from... but this is battlefield triage, you'll live without hospital therefore you're mild to our eyes right now. When we're out of this emergency you will have the luxury of calling that mild illness "severe" and we'll go along with you again.At what stage should a person contact the emergency services for help? What fever in adult and if they find it hard to breath?
I'd definitely call a doctor if I was having significant shortness of breath unexplained by any other underlying illness.Would keeping track of BP and Oxegen levels help emergency services decide whether you need hospitalisation? (Oximeter readings)
Yes, my parents have a blood pressure monitor and thermometer and I made sure they bought a pulse oximeter in the run-up to this. I have instructed them that if they think they might be unwell to take their blood pressure and oxygen saturation every morning and record the results on a different sheet of paper each along with the date.
That way they'll be able to tell me and/or their GP their routine obs over the phone and it'll help establish that they're not just anxious as well as creating a timeline of any deterioration in their health.
I have the same and will post my temperature, oxygen saturation and BP if/when I get COVID-19.Asides from being tested will a lot of people with “mild symptoms” possibly not ever know that they had the disease unless for some reason they are tested? Is it possible in the future to be tested to see if you had it or have antibodies?messinkiapina wrote: »For individuals who experience mild symptoms to the point they may not even know they've contracted it (and presumably develop immunity afterwards), will testing be available to them at some stage? And would those tests show that the virus had been present but overcome?
It would be ideal if everyone who's had this knew about it, they could stop social distancing and help the vulnerable and those in need of care?
Yes, that should be possible but will be a luxury we only have once we've largely beaten this, have enough test kits to test new suspected cases + a surplus and are trying to return to normal.
I can see the value in being able to re-assure people that if they go out and about they are likely to be immune to the circulating strain.Drugs to treat malaria and arthritis have been showing positive signs in treatment. Will these be available in Ireland if required?
Thank you for your help in uncharted territories. Keep safe.
Well any medicine which shows promise will have some availability in Ireland. E.g. some anti-HIV drugs have shown promise. We have about 5,000 individuals living with HIV in Ireland so we have supplies commensurate with treating those 5,000 individuals. Let's imagine an anti-HIV drug was proven to cure COVID-19 100% of the time... but we have 200,000 infected per month with 20,000 needing hospitalisation and thus being ill enough to need the drug.
You now have 25,000 people who need that drug per month. Even with unlimited money the companies which make that drug didn't build 400% additional capacity a year ago just sitting there wasted so while they can increase production there is no way they can increase it to 25,000 in a matter of weeks.
So, doctors have to make choices, hard, hard choices of who will live and who will die. I refer you back to my previous post about stained souls and minds and the mental health fallout.
Of course the more you socially isolate, distance and handwash the lower the peak in infections. If it is 50,000 instead of 200,000 and we have 5,000 who need hospitalisation a month then we can probably figure out a way to stretch supplies to those 10,000 people and save a lot of lives. That is where you, the public, come in.
And that takes me to the bottom of page 3. I'm going out to run supplies to the parental units. I'll do the 4th page on my return.0 -
Cork Boy 53 wrote: »I am just curious as to whether you think a time may come when a virus or some type of infectious disease will appear that will have the potential to effectively wipe out all of humanity. I`m talking 12 Monkeys style here. Hopefully this one won`t be it! Anyway my thoughts and prayers are with you and your colleagues for the ordeal that lays ahead of you.
Wow!!! and my posts are accused of increasing anxiety ;-). I think that over the past two decades we've had Swine Flu, SARS, MERS and now SARS-CoV2. That's pretty much one pandemic or potential pandemic every 5 years.
Unless we change our relationship to the planet I see no reason that that pattern won't continue but if we continue to fund vaccine research and pandemic prevention planning beyond the current crisis I think we won't be wiped out by one.
With that said on a philosophical level I agree with Elon Musk that so long as humanity exists only on one planet that planet represents a critical vulnerability for the human race and so the sooner we get self-sufficient colonies on other planets the better. But that's more a philosophical point than the death knell of humanity in the next few months. Even the absolute worst case scenario for SARS-CoV2 won't wipe us out or reduce human civilisation to Mad Max levels") .Funnyonion79 wrote: »My question is this...in two weeks time, after self isolating at home with my husband and children, is it safe for us to visit my parents/in-laws, who have also been self isolating at home, during this time? The only time any of us would've left the house is to go for a walk or go to the supermarket. The in-laws are mid 70s but in good health.
.Funnyonion79 wrote: »My question is this...in two weeks time, after self isolating at home with my husband and children, is it safe for us to visit my parents/in-laws, who have also been self isolating at home, during this time? The only time any of us would've left the house is to go for a walk or go to the supermarket. The in-laws are mid 70s but in good health.
Well, I am not trying to dodge the answer here but I don't think there's a simple yes or no answer to that. Certainly after two weeks of self-isolation your risk of being infected without symptoms is low but it isn't zero. And going to the supermarket definitely creates a risk of infection.
My position with my family is that I'm dropping things at their door and picking things up from their door while the door remains closed. We wave at eachother through the window and talk on the phone or via skype. I think that's the safest way to proceed.
You can certainly go and visit them but that introduces a bit more risk and only you can balance that risk/benefit ratio for you and your family. Either way I wish you the best.JustAThought wrote: »Still wondering where the answers are, please - is there a link?
Q: While front line staff paid are being allowed home on paid sick leave inc to mind their children off school unpaid inexperienced volunteers are being emailed from the HSE asking them to go into hospitals to help with the virus. Something fundamentally wrong with this. Surely the time for paid HSE staff to pull their weight is when there is a crisis and they are needed and not be asking or relying on emailing randomers from a charity database to pick up their slack.
My family member called in sick on full HSE pay to mind her children - surely this type of abuse should be stopped.
I'm not an HR professional so cannot address this but I do know we've all received memos stating that the HSE is recording who steps up and who doesn't at this time. You don't have to be a genius to figure out what that means for people who are adjudged not to have made themselves available when they could have. With that said individual circumstances are often highly personal and I'd be slow to rush to judgement. There may be stuff going on you aren't aware of ( undisclosed medical conditions etc ).
So, my general policy at this time has to try to be kind and thoughtful and not jump to the assumption that people are shirking... but I'm sure those cases will be looked into afterward.
@Purgative,
Thanks. I'm glad to hear you found my answers of some value and hope those you shared them with find them helpful also.How long is the recovery period?
I think that depends very much on the severity.
1. It seems that most "mild" cases ( meaning not requiring hospitalisation ) should be fine within less than a fortnight... and may just need to self-isolate up to 14 days to make sure they're not shedding the virus even though recovered.
2. I've seen figures from China and Italy which say the 10% who require hospitalisation but not ventilation can take somewhere from a week to a month to be fit for discharge. The median reported by Wang was about ten days.
3. I've heard figures of about a month being quoted as the average for patients with severe illness requiring ventilation but I think that figure will change as we get more data from more recovered patients.What is the protocol if a work colleague tests positive? Is the work place contacted? and if so by who? What happens after that?
I think that advice has changed a few times based on exingent factors and developing medical understanding over recent weeks so I'll answer with two general points:
1. The affected individual will be contact traced by the HSE as per their protocols.
2. If you haven't been contacted but are concerned you can phone your GP who can assess you and determine whether you meet testing criteria. Follow their advice as it will be individualised to you and thus be higher quality than any general advice you can get on the internet.It was a disease running around late December/early January. In reports from that time it was said that there was a 25% increase in hospital admissions of patients over 75.
So my question is: how HSE ruled out that it was not Covid-19? How many tests were made to prove it was something else like a different kind of flu (I mean percentage of cases checked for it)?
Not in Ireland it wasn't. The phylogenetics of SARS-CoV2 show it wasn't in Ireland at that time. This is an unhelpful assumption/internet rumour not supported by facts.
I'm sure the seasonal flu was around and quite a few people got sick and died from it, as they do every year. But it wasn't SARS-CoV2. Check out the link I've provided above to look at the genomic epidemiology yourself. The phylogenetics speak for themselves.
I hope you find this answer helpful and can put this unhelpful internet rumour to bed.Hi there,
Have you seen any day services cancelled ? My OH has MS and is on a monthly infusion. As far as I understand there is a massive increase in the risk of an attack if left for more than 5 weeks between treatments.
Have you seen or heard if any alternative arrangements for these treatments ?
I think that, whenever possible, essential services will continue to be provided. With that said if we have 20,000 cases a month the number of normal services we can decide are essential will be a LOT more than if we have 100,000 cases a month.
So, again, it comes down to social isolation, social distancing and handwashing. The best thing any member of the public who is worried about a relative with treatment which may be cancelled is work to reduce the spread. That gives the greatest chance that we will have the staff and space to continue these sorts of services.How do you feel about the speculation happening that health care workers are at much higher risk of developing severe/critical illness if they come infected? Have you any advice for other front line hospital staff?
I am not familiar with this speculation. Healthcare workers on the front lines, doctors, nurses, cleaning staff etc get infected at higher rates than the rest of the population but I'm unaware of any increased mortality rate ( as opposed to absolute mortality ).laserlad2010 wrote: »If you're not a public health specialist you have no business providing official COVID-19 advice, even cloaked as personal advice, to the public. It's bad enough with the Whatsapp rumours, but talking about writing your own will at the same time as attempting to give advice in your capacity as a consultant is inapproriate. Regardless of whether it turns into a "war".
Even if you claim you're not representing the HSE people will still place weight on your words.
I've been explicitly clear that I'm posting in my personal capacity informed by my training and experience. It isn't my problem if you cannot read and say I'm "providing official COVID-19 advice".
As to the will. It is what I've done. It is a sensible precaution.Maybe we should ask him if threats like Covid 19 show the impracticality of organising access to medical knowledge through a tiny bunch of highly paid consultants. I think he'll know what we mean.
I actually don't know what you're getting at. I'm assuming it is some sort of class warfare dig at Consultants which makes the mistake of thinking that being able to google a thing and UNDERSTANDING IT enough to be able to make really difficult decisions are the same thing. They aren't but, you know, you do you.
What I will say is the two of you amply demonstrate:
a) that some people still don't understand what we're facing and
b) why I want to remain anonymous. You're the sort of people I don't want to run into in the real world.
With that said I wish you and yours the best of health into the future.Thanks for taking the time to do this, I think it really helps to have good information out there as much as possible.
1. How soon do you think the number of infected people in Ireland who need treatment will reach a level where the health service is finding it hard to treat them all?
This is a really great question actually. It gets at the heart of a lot of confusion out there about models and probabilities - and humans are really bad at understanding probability.
What doctors and the state have are models which show what estimated numbers of infected will be based on various levels of social isolation, distancing and handwashing as well as curbs on flights, pubs etc.
In simple terms the outcomes of those models range from - "Oh that wouldn't be too bad" to "Oh S**t!!!". The more the public socially isolates whenever possible, socially distances whenever going outside is essential and hand washes the closer we'll get to the "Oh that wouldn't be too bad" level of outcome.
I've heard reporting on the radio that the government is estimating there could be 10,000 to 15,000 cases by the end of the month, two weeks from now. If we assume 10% may need ventilation that would be a requirement for 1,000 to 1,500 ventilators. We have about 250 although as explained previously we can repurpose more. That's pretty grim.
And, yeah, you guessed it the best thing you all can do is socially isolate, socially distance and handwash.2. I've seen reports that asthma may be a risk factor because Covid might exacerbate the asthma, but the actual Covid illness itself isn't necessarily more severe. In other words, the claim is that the main extra risk to people with asthma is that they will end up with both Covid illness & a severe exacerbation of the asthma, and therefore the additional risk for people with mild asthma is probably not much greater than people without asthma. Is this likely to be accurate or not?
I think that gets into an unnecessary level of detail of disease action which we just don't know yet. It appears that anyone with a chronic respiratory illness is at increased risk of mortality. It certainly seems reasonable to assume that someone with COAD is going to be at more risk than someone with mild asthma well-controlled with inhalers but I simply don't know that for certain at this stage and certainly don't know any figures I could quote which I'd consider reliable and solid.
I can provide you two links which could be useful:
1. UK Asthma Organisation advice page. This seems solid to me.
2. Irish Asthma Society's page. The UK one seems better to me honestly but I provide this for the Irish perspective.
In this situation the best thing to do is read those organisations' websites and if you have further questions/symptoms seek advice from your GP or treating Respiratory team.0 -
Sour Lemonz wrote: »My eldest nephew (age 11) has cystic fibrosis, my sister does all his IV's at home, he is on orkambi, lung capacity up and all good stuff at the moment. However with the virus going around there is obviously a concern for him as lung functionality could become an issue. He is very good at washing hands and looking after himself like meds for his age, but there are going to be times where he cant control a situation and may pick this virus up.
Some advice that was given to me today (cant confirm person is a health professional) was that if my nephew showed symptoms then get him to a sauna 2-4 times a week for 30 mins at a time that and the heat and steam of the sauna would kill the virus as it lodges in eyeducts, nasal cavity. Is there any truth to this ?
I would be astounded if any health professional gave that "advice". That sounds like extraordinarily dangerous and unhelpful advice.
If your nephew started showing symptoms you should contact your GP and his specialist treating team as a matter of urgency. There doesn't seem to be much definite information about individuals with Cystic Fibrosis being infected with Coronavirus as it is relatively rare worldwide. I wouldn't assume that means it'll be a mild illness if they're infected. I'd socially isolate strictly out of an excess of caution. Better to be too strict with self-isolation and then relax it than to be lax now and regret it down the line IMO.
Here's information from Cystic Fibrosis UK
Uk Cystic Fibrosis Trust Q&A page
Cystic Fibrosis Ireland hasn't updated their info in the last 5 days and I believe events have moved on significantly since then. Here's a link to the latest advice from them.
If you are unsure what to do you should contact your GP or treating specialist and receive individualised advice for your nephew. I can't give individualised advice for your nephew. I just know what I've said to patients of mine with CF or those with relatives with CF.0 -
Join Date:Posts: 70125
A reminder - this thread is for the AMA answers only. Questions should only be posted in this thread0 -
Advertisement
-
To those who have contacted me re: 3D printing links...Thanks, I'll pass it up the chain just in case they aren't pursuing that line yet.
I have an image I edited on my computer I want to upload. Does anyone know how I can upload it to boards or somewhere else so I can link it here in this answer?I watching a UK parliament committee asking about the lack of appropriate PPE for medical staff on the front line of the NHS.
How are medical staff fixed for safety equipment in treating patients.
Well, I don't think any health service has enough PPE for their staff given what is coming. We are awaiting deliveries of new supplies and I'm sure production is ramping up massively worldwide and China will be able to provide masses of PPE once they have their outbreak under better control.
It is a worry but not treating people isn't an acceptable option. In Italy when they ran out of masks etc they just worked and got sick. Then they kept working until they got too sick to work and became patients themselves.
I'd expect no less will happen here. But the more time the public buys with social distancing, isolation and hand washing the more likely we are to avoid such a scenario.Fishorsealant wrote: »What do you think of the situation regarding dentists?
One of the professions most at risk yet very little guidance available. One of the last professions to be considered despite providing an essential role and being at high risk.
Many dentists taking it on their own to decide whether to open or close.
Do you think forced closure except for emergency treatment would be wise?
It seems to me that dentistry is a pretty close proximity job. If I were a dentist I wouldn't risk it. I think it would be helpful for them to receive official guidance but it seems many of them are doing their own risk assessment and deciding to close already without official advice. Obviously though I can't tell dentists what to do. I just know I wouldn't take the risk were I a dentist.
I'm sure some public dentistry will remain open for real emergencies for the duration.Away With The Fairies wrote: »Keep hearing that the majority of people will get through this fine at home?
Do we ring doctor on day 1 just to make them aware that you're not feeling the best?
I think that would be reasonable so they can arrange for testing and confirm whether this is COVID-19 or just some more common garden bug. As we have more testing kits available we will be able to test more widely.
@JoChervil
The phylogenetics of the Irish cases doesn't appear to support what you suggest... but people believe what they want to believe. I'll try to add a picture illustrating that one of the cases can clearly be traced to a nexus from the Netherlands in late February.
That's what makes this type of analysis so powerful, you can see how closely related viruses in individual people are and build up a picture of where they came from and how long they circulated.
If it had been here since 2019 we'd see the phylogenetics of Irish cases being far less closely related to other European cases from 2020 than we currently see.
The science of European cases simply doesn't support your assertion and it is clear that Irish cases are related to these recent European cases. It is your choice whether or not to disregard the scientific evidence though.
Either way I wish you and yours the best of luck at this time.No questions..Just to say well done to you and you're fellow front line staff....
From the description you gave of you're own self imposed current isolated lifestyle it should be enough to make people aware as to just how serious this threat is..
Myself:- Legionnaires disease 10/'19...COPD..Smoker...SO I realise the limitations of my survival through this and have already come to terms with it..will not be expecting to tie up an incubator....
Well, let's both try to be extra safe then and wish eachother a Happy Paddy's day this day next year eh?Thank you so much, it’s great to have so much information in one place. I’m just wondering, as A & Es become overwhelmed with this - will there be seperate areas for people coming in with other problems. Thinking of elderly parents having middle of the night heart symptoms or similar. Would letting people wait in cars be an option?
This is what they've done in Italy and China with A&Es and their hospitals. They've segregated COVID-19 and non-Covid-19 patients as much as possible to keep the non-COVID-19 patients from becoming infected. Similar segregation will happen here. How it will be organised will change depending on local factors obviously.AndrewJRenko wrote: »Thanks for your inputs, very helpful, and thanks for your ongoing work.
What's your understanding of the risk of outdoor activities, particularly for teenagers? Is there risk arising from a brisk walk, or a chat at a picnic table outdoors? Mental health is a real concern, and they do need to have some contacts outside the family circle.
I think you'll have to decide how you want to balance that risk vs benefit individually. Obviously then going out at all is more risky than them staying inside and just skyping their friends.
I think a walk outside is pretty low risk all things considered so long as you aren't in a group or stopping to chat to others but a chat at a picnic table or anything else which resulted in close contact isn't something I would see as a good idea.
They may not like it but just give them unlimited screen time and the right to skype their friends as much as they wish 0 -
Quick answer to something and then some links...
1. I think the best preventive measure is total social isolation but recognise that isn't possible for most. So, going for walks is a calculated risk.
Ideally if you're going for a walk it should be alone or only accompanied by whoever you are in social isolation with ( partner, children etc ), you should avoid other groups of people and do your best not to touch anything with your bare hands - e.g. door handles to apartment buildings, lift buttons, gates etc -- which others who might be infected might have touched.
Those steps should reduce the risk significantly. So, in summary, going for a walk when lots of people are around and having chats with them while touching door handles, lift buttons, gates, then popping in to the local shop to pick up a coffee all increase the risks.
Going out for a walk with your partner and/or kids when/where there aren't large groups out walking, having a walk, taking care not to touch things with your bare hands others may have touched and not stopping for chats - even if you stand 1 metre apart - all contribute to a walk being a low risk.
I happen to have a treadmill at home and so I've made the decision to only use that from now on but I recognise that isn't an option for most people.
In other news I've been contacted about Remdesivir and other potentially effective treatments and I think it would be worthwhile to curate a post with links to scientific journals about possible treatments. I am NOT endorsing any treatment or anything like that, just hoping to:
a) provide a little hope
b) provide links to actual research articles as opposed to whatsapp rumours and
c) provide a short summary ( a couple of paragraphs which are simplified and should be easily understood ) so as to "translate" from "medical" to English ;-)
Let me know if you think this linking to research is useful or not. If not I'll find better ways to spend my time.
1. New England Journal Of Medicine Case Report of US Male with COVID-19 successfully treated with Remdesivir.
Basically a patient who was in Wuhan and then returned to America tested positive for COVID-19 and was then admitted to hospital. They received supportive care (paracetamol, ibuprofen, saline) for the first 5 days of hospitalisation. On Day 5 their Oxygen Saturation fell below 90% ( anything below 92% is significant in a previously healthy person ) and they were started on supplementary oxygen ( the nasal prongs or oxygen mask you'll often have seen people on in hospital ) and antibiotics for query hospital acquired pneumonia.
On Day 6 their chest X-rays were showing worsening lung involvement and the doctors applied for "compassionate use" of a the drug Remdesivir ( a known antiviral which had been trialled in the treatment of Ebola in 2019 but didn't do well ) and started it on Day 7.
By Day 8 the patient was improving.
Conclusion: Remdesivir may have utility. More evidence needed. A single case study so hardly proof positive of a treatment for all. Still, a damn sight better than giving it to someone and them not recovering. We WILL find existing medications and/or new medications which work to kill the virus and then survival rates will improve markedly. It is just a matter of time. Buy us that time with social distancing, social isolation and handwashing.0 -
mrsherself wrote: »Hi!
I was just wondering - I know best advice is to stay inside, but for those of us who will end up going mad, is there anything wrong with going for a walk outside by yourself?
Is it not a good idea to go to a park where there will be other people?
Well, exercise is good but the trick will be not exposing yourself to risk by being around others so if I were going out for a walk I'd take care not to run into others, stop for chats or touch things others might have touched. Those are the real danger points.My wife and I are in our late 60's. She has well controlled bronchiectasis for c.5 years and I was hospitalised and successfully treated for septicaemia around then also. No major issues, both in good health and walk daily. Would either condition mean a greater risk of complications if we got infected?
We are taking all recommended precautions and don't expect a medical opinion, just any general views you feel you can offer.
Yes, I don't want to get into giving the impression that I'm giving individualised medical advice as that isn't really appropriate over the internet. The best bet is ALWAYS to phone your GP or treating specialist and ask them about your individual case. With that said while septicaemia is generally once and done I believe the vast majority of doctors would classify bronchiectasis as a chronic respiratory condition. We know chronic health conditions increase the mortality of those infected with COVID-19 so I think it would be very sensible for you and your wife to be exceedingly careful and very strict in your social isolation.
I hope that helps give you actionable information.Sober Crappy Chemis wrote: »Realistically, is it a big risk to go to a supermarket or pharmacy obeying physical distance etc, if one has asthma and is also immunosuppressed?
Well I think immunosuppression clearly puts you in a high risk category and supermarkets and pharmacies are places people congregate. I wouldn't be taking any avoidable risks if I were in a high risk category. I have two underlying conditions which increase my risk of mortality and if I weren't in the health service I would simply be staying at home, having my groceries delivered by Tesco/Supervalu/Lidl/local shops and would be asking the pharmacy or a younger relative to pick up my prescription and drop it at my door.
I don't have that choice and so am out and about because I have to go to work, fill the car etc but I only do those things because they are unavoidable and I'm very conscious that being out and about significantly increases the risk of me catching SARS-CoV2. For those who aren't in essential jobs I just don't see the point in taking those kinds of risks.
Obviously we're all adults here and have to balance the risks vs benefits for ourselves and you might decide that balance lies in a different place than I do.This question and answer thread(s) has taken me completely away from the main rumour and conjecture thread. It has done wonders for my well being with regards to worry. Yes I know it’s coming and unavoidable but the main thread lacks the sanity in these.
Thanks, I'm glad it has been helpful to you in that way. Later in the week I'll get to posting some maintaining your mental health advice gleaned from colleagues etc as I think that's an important aspect for people also.Thank you for your informative and reassuring answers so far.
What is your opinion of small children (aged 5-9ish) playing together in small groups on driveways/on the road while doing their very best to maintain social distancing; children who play together everyday and who, under normal circumstances, are in and out of each others houses almost everyday. They wash their hands immediately after coming in, and door handles etc are cleaned regularly throughout the day. Are they putting us, their parents, at risk? They are isolated from everyone other than their own parents and those few pals. Is this behaviour potentially speeding up the spread?
Yes, they are absolutely putting anyone they come into contact with at risk. Kids playing together simply will not maintain the necessary social distancing and no touching rules and so the risk of one child infecting the others is high. Those other children will then bring it home to each of their families who then have a high risk of becoming infected.
I saw this happening where I love repeatedly on Paddy's Day. There were groups of 4 and 5 children playing outside. Some of my colleagues reported seeing the same. We all thought it was insane behaviour by their parents to let them out like that. If you allow the kids out like that then you should absolutely expect the entire family and road/apartment building to become infected sooner rather than later.
Social isolation means just that... It doesn't mean seeing almost no-one but having the occasional dinner party or play date. You should do it fully or not at all because half-assing social isolation will simply not work.
Hell, I have to get diesel for the care and I'm going out after I finish this post ( about 2:30am) to an all night garage because I'm awake and assume that there are a lot of asymptomatic spreaders out there and if I go during the morning rush hour I'll have to contend with a lot of people paying in the shop at the same time. Now I wouldn't stay up purposely till 2am to make that run but I definitely planned, today, to do the run in the middle of the night as I knew I'd be up so as to avoid social contact as much as possible.... and I'll fill up with more than 30 Euro so can't use contactless payment... so I'll be buying 50 Euro of diesel and handing over a 50 Euro note so I won't have to receive change or touch a credit card machine. Sure, it sounds paranoid but once the deaths start occurring in large numbers more and more people will think that way. I'm just basing my decisions on where I know we'll be two weeks from now rather than today. For me, being infected really is a matter of life and death ( about 20% chance in my estimation ) so I'm taking it pretty seriously.up for anything wrote: »I met a friend I haven't seen for a couple of years the other day. We were chatting about our children, one 'stranded' on a Spanish island and mine just home. I asked her kind of tongue in cheek about what her husband, a fairly senior detective locally, and his colleagues thought of the whole Covid-19 'business'. She replied that his job description had been changed to one thing, just the one thing. When I asked her what, she replied, "transporting dead bodies". From what the undertakers were told and from general knowledge I know that the bodies of those who die of Covid-19 will be hastened to the crematorium and into the ground as quickly as possible and will need people to be responsible for the process. However, the way she said it and the look on her face seemed to say volumes. Are you expecting many people to die in the next couple of months and what is the figure? I assume a figure must be available from the data from other countries and applied to Ireland. Morbid question, I know.
Well no-one knows how many will die. We can make estimates. For a few weeks now I've been saying that my optimistic best case scenario is about 1 to 2,000 dead over the next few months. My reasonable best case is about 5,000 dead. My pessimistic best case is about 10,000 dead . You really don't even want to hear the middle and worst case scenarios.
With all of the steps the government has taken I am confident we are bending the curve towards these best case scenarios rather than the middle and worst case scenarios. I think it all really comes down to how the public behave. If the public actually practice social isolation instead of "social isolation with a splash of dinner parties or kids playing etc etc" then I think we'll be closer to the optimistic best case scenario. If the public are cavalier about social isolation then the death rate will be much higher.
Right now the public has the ability to save far more lives than the health service by practicing ACTUAL STRICT social isolation, instead of an approximation of it which isn't actually it.
But while I see some people taking it very seriously I know friends who have gone into work and worked directly beside others ( the other person is now a suspected case and my friend is in self-isolation awaiting symptoms. Since exposure they visited a sibling who has also now been exposed and that sibling is now visiting their parents who both are in high risk groups... that's not social isolation, that's just being stupid. I warned them last week when they told me their plans but they went ahead anyway. It could cost their parents their lives. ), who go to supermarkets without gloves and masks and use the same trolley that a dozen other people pushed that day ( SARS-CoV2 has been shown to survive on plastic surfaces for more than a few hours ) etc. All of those people have told me they are following all the advice and socially isolating but in reality they aren't, they're still doing things which pretty much ensure they'll be infected and they mistake sitting at home in the evenings as being social isolation. It isn't.
But in my job I learned long ago that people only listen to what they want to hear.up for anything wrote: »Oh, another question, if you don't mind. People with Diabetes are very much at risk apparently. Is it more those with Type 1 or those with Type 2 or those who have Diabetes which needs to be treated with insulin rather than Metformin/exercise/diet. Are Type 2s with just over the borderline sugar levels, more at risk than someone without it. If you're not sure, would you be able to point me in the direction of some information please and thanks?
Again I don't want to get into individualised advice but what I can say is that the Chinese figures we all are working off didn't, to the best of my knowledge, differentiate between Type 1 and Type 2 or whether it was well controlled or not. They just say that if you're diabetic you have a much higher mortality than if you're not ( independent of age ). So, I would simply take it that ANY and ALL diabetics are in a high risk category and should exercise strict social isolation.
Here's a decent summary medscape article.... I would caution though that while they seem to say that how well controlled your diabetes is could play a factor ( better control leading to better outcomes ) it is early days and the best way to play this is to assume the diagnosis makes you high risk no matter how good your control is and be very strict with your social isolation accordingly.Gentleman Off The Pitch wrote: »There are reports of people successfully overcoming the fever after a few days, only for them to be hit with severe shortness of breath and pneumonia a few days after that again.
Are there are warning signs of this occurring and are there specific instructions for people who suddenly find themselves in that position, particularly those in the at risk category, so that they make the correct decisions and attempt to get appropriate help as soon as possible?
If possible have a thermometer and pulse oximeter and begin recording them once a day when well. Then note when you feel you might have been exposed and keep an eye out for any deterioration. If you see the oxygen saturation fall significantly after you think you might be infected then I would call the GP and describe the symptoms as well as the timeline of exposure and changes in temperature and oxygen saturation.
That'd be the best situation and how I've advised my parents to deal with this. If you don't have a pulse oximeter then I think you need to call your GP if you think you might have symptoms indicative of COVID-19. Your GP will then assess and advise you appropriately.On underlying conditions - I have had a heart bypass, 10 years ago, 54 now, in good shape generally, did a 13 minute treadmill test a month ago and had follow up with cardiologist in Mater. Hit 100% max heart rate, etc, so cardiologist was happy with the performance.
Just wondering if a bypass fixed the heart issue, is CVD still a reason to self isolate when the time comes with my underlying condition? Am I at the same risk as someone with COPD, heart failure etc, or can I go about my business?
I know the bypass fixed the problem, and the disease still exists. Hence my question, mortality rate for CVD is quite high, seemingly 13%, so I have that concern of course.
Thanks in advance.
Thanks for the question. It sounds like your Cardiologist is right to be happy with that performance. Well done.
I would take a cautious approach to this and say that until proven otherwise I would consider having required a heart bypass to represent underlying cardiovascular disease and thus I would consider myself to be in a high risk category if I had required one. That would be my general, "better safe than sorry" approach.
However with that said I recommend you contact your treating Cardiologist and ask them this question. They will know your individual circumstances and history better and thus be able to give you an individualised answer which will take into account the myriad other factors which impact this.Many thanks for both this thread, and all the work you are going to be doing over the next period of time. Stay safe.
For those of us with underlying conditions, with regard to Leo's speech last night, he mentioned elderly and vulnerable and cocooning. Do you have any idea how we are going to identify whether our underlying condition is sufficiently risky to warrant this when we are not elderly?
The graphic on page 1 of the answer thread shows some of the main risk factors which increase mortality. Bottom line though Hypertension, COAD, Cardiovascular Disease, Chronic Respiratory Illness ( this could include asthma, bronchiectasis, existing fibrotic lung disease), Cancer, Epilepsy and other underlying neurological illnesses, Diabetes all seem to increase your risk of mortality significantly irrespective of age.
With that said this illness is so new that we are constantly learning about it and two things I'm certain about are that:
a) Not all things we think are true now will remain true 6 months from now.
b) There are many things we simply don't know about it at all which we'll know 6 months from now.
So, we don't know everything that increases risk. 6 months from now we'll know much more precisely what illnesses increase your risk. So, right now you have a choice between being cavalier about your health and assuming a chronic health issue doesn't increase risk and being cautious and assuming it might and thus being stricter with your isolation. Some illnesses ( the ones I listed above in the answer ) are ones we are pretty certain increase risk. Others we simply aren't sure of.Asking for a friend ��...There’s lots of us here with partners working in the healthcare system ( me included) What precautions do you take or recommend when coming home from work to protect your own family
Well the best thing they can do is just follow all of the infection control advice at work, ensure they have the right PPE gear, take the time to work smart etc. Also a lot of healthcare workers in previous viral outbreaks have gotten infected via community transmission not transmission from sick patients at work so while your partner should be careful at work you all need to be careful at home/in the community because that's actually a surprisingly large vector for infection of healthcare workers.
One thing I'd definitely say is they should leave all their workwear at work to be cleaned there and chance back into "community clothes" in as close to a clean room as they can manage at work. That way the only thing you bring home from an infected ward is your body --- which should have been protected by the PPE gear.DevilsHaircut wrote: »Should we be making it completely and unambiguously clear that SELF-medicating with anything for Covid19 symptoms will do nothing to fight the actual virus?
https://www.boards.ie/vbulletin/showpost.php?p=112861398&postcount=5158
RANT MODE ENGAGED. Oh FFS!!!!! My patients do this all the time. Deciding to chop and change medicines, increase or lower doses without bothering to phone my service first and then phoning weeks later when their health has acutely deteriorated. I'm not an electrician so I don't decide to rip all the wires out of the walls at random times and try cross-wiring them cause I think I could do better.
Medicine is complicated. Self-medication based on almost complete ignorance of how drugs interact and work is a wonderful way to save the virus the trouble of killing you cause you'll do it to yourself.
Now, obviously if you've got a temperature and you aren't allergic something like Paracetamol seems safe enough based on the evidence we have but apart from that I'd be phoning the GP. Hell, I'm on medication which deals with an underlying condition outside of my specialty. I NEVER tamper with it and I sure as hell know a lot more about medicines than 99% of people reading this thread. If I KNOW it is such a damned stupid thing to do that I don't even touch it with a ten foot barge pole just what the hell are any of you considering it for.
Seriously, I've seen quite a few patients die from self-medication. Don't do it.Hi again Psuedo,
just a question that came up over on the Diabetes thread. As Diabetics are a high risk group as per the advice from Government/WHO, many of us are taking all available precautions.
is there however any difference in the advice for T1 and T2?
Or is it a blanket advice?
My own understanding of T1.5, T2 in particular is that as inflammation is a particular risk in any event that it should be a case of isolate and stay safe?
Does one's control have any bearing?
or is it really a case of suck it up, mitigate and isolate?
It really seems to be blanket advice for T1 or T2. As to control... we don't have the evidence yet to definitively say whether better control leads to better outcomes with COVID-19. With that said better control is just a good idea anyway so aim for better control cause that's a good thing in general but assume no matter how good your control or whether it is T1 or T2 that you're in a high mortality category.
I hope that helps inform your decision making.celticWario wrote: »In relation to claims by a HSE whistleblower that the current state of hospitals are "filthy", has there been an effort to deep clean our hospitals in the past few weeks in preparation for what's to come?
https://www.dublinlive.ie/news/dublin-news/coronavirus-filthy-hospitals-wont-able-17884118
Well I don't know all the specifics but this person sounds quite extreme and out of touch with the realities of the situation. Calling the army in to do a deep clean would be both ineffective and impractical. It makes me wonder just what their experience and level is. You often hear this sort of thing from relatively junior people who think that a certain thing is wrong and then lose all perspective. This reminds me of that sort of situation.
The army has NO particular experience, ability or equipment necessary for a "deep" clean. Certainly they don't have the ability, experience or equipment necessary to deal with CPE. There are specialist firms which do that.
Additionally I don't think a "deep clean" would be of any great value now. In fact I'm certain it would hamper preparations far more than it would provide any benefit. So, really, I think that that is unhelpful, wrong and harmful. Whoever this person is I'm not surprised their management don't listen to them.mariaalice wrote: »If someone suspects they have the virus but are generally well and have painkillers at home and they decide to stay at home for two weeks and just get through it.
Do they need to get tested or can they just stay at home?
I think they should contact their GP and follow the advice of their GP. I think once we get enough testing kits it'd be useful to be tested to know they had COVID-19 as once you know you have it you should be able to interact freely in society again without fear --- until/unless a new strain develops. I think knowing you had it and thus being able to go out freely again would be well worth having the test done.How can we help? At the moment we are taking this seriously and avoiding all unnecessary contact with others. We do ring older people to see if they need anything but they have been ok so far. When things get worse, will there be volunteers needed or is continuing to isolate the best thing we can do?
Edit: Do you think things like this interactive map connecting volunteers with the self-isolated are a good idea?
https://www.limerickleader.ie/news/community/526492/interactive-map-connects-volunteers-with-self-isolated-in-limerick-during-covid-19-crisis.html
I think the MOST important thing you can do is socially isolate, distance and hand wash and convince friends and family to do the same... STRICTLY!!!!
Next I think anything whereby we try to help others helps us all. I am responding to these questions at 3:23 am because I felt this was the best way I could contribute outside of my day job. I think other people should ask themselves how they could best contribute. That might be volunteering or it might be the HSE "Be On Call For Ireland" campaign ( link included )Quick question regarding self-quarantine, should someone whos in remission from hodgkins lymphoma for just over a year and received 6 months of ABVD chemo be travelling into work on public transport & work in a busy office in the city centre or do they fall under the at risk group advised by HSE to self-quarantine?
We don't know the answer to that yet. We know that if you HAVE cancer or are receiving treatment for cancer then you are at higher risk of mortality.
I haven't seen any solid data about survivors of cancer who aren't currently on treatment.
However I have been advising people I know to avoid public transport if at all possible - unless they wear gloves and a face mask - because why take the risk? People and crowds are dangerous now. There are lots of people in public transport ( buses, dart etc ) and they touch everything. Also the ventilation usually isn't amazing. So I just think they're to be avoided if possible unless you have gloves and a really good N95/FFP2 mask at least.
I can't prove that with research but that's certainly the route I've advised friends and family to take... but I'm advising a lot of caution around this as I think this is going to be worse than most people think even now. I would LOVE to be proven wrong on that though. The wronger I am the more people live so I'll take that trade all day long.Call me Al wrote: »Thank you for your guidance, and the work you and your colleagues will be doing.
Your last post said this:
"It is just a matter of time. Buy us that time with social distancing, social isolation and handwashing."
Do you think we are doing enough?
My household is doing absolutely everything by the book but its frustrating as hell when I heard about people going to house parties last night and kids like my own on playdates who are all unable to self-regulate the social distancing.
I called my health insurer nurseline about information I'd read, (both media and scientific journals) about ace inhibitors and concerns surrounding these. I was told that their medical teams were aware of this and that there were many uncertainties. Now I'm not coming off the medication or anything extreme like that, and I did contact my gp with my questions, which we all should do!
Is there any verifiable science surrounding these medications and their interactions with covid19?
I think the public don't get it yet. I think they'd look at the precautions I and my family are taking and thing I'm some sort of crazy prepper. But I'm just someone who did the maths weeks ago and started raising the alarm weeks ago and is behaving based on where we are going to be 2 weeks from now and 4 weeks from now rather than where we are today.
These play dates and dinner parties etc honestly annoy me. They are spreading SARS-CoV2 and by doing that are condemning citizens of the state to death. It is THAT simple. I think it is incredibly foolish and selfish behaviour.... but I also understand that most people doing that sort of thing aren't bad people, they just haven't really come to terms with the seriousness of the situation. It'll take an increase in death toll in Ireland to get them to change their behaviour... but in the interim they'll keep spreading it ensuring more die than necessary and overwhelming the health service more and more.
They'll probably also be the ones b****ing about the health service and governments' failure to protect them when this is all done. I could say more but I'd just get really annoyed and that'll do no-one any good. Plus it is time for me to do my run to partially fill the car.
I'll be back tomorrow or Friday to answer the remaining questions.
Best of luck to all.0 -
RiseAbove4 wrote: »I’ve been reading your posts with both interest and high anxiety. I believe all your facts and thank you for doing this.
Question:
I’m a 44 year old male with Cerebral Palsy. In addition I’ve early Osteopenia and I’ve picked up some kidney stones in the last couple of years. I’m also allergic to Penicillin which is used to fight off lots of bugs. .
My CP is mild compared to others. I can still walk and I try to exercise as much as possible.
Am I at any higher a risk than another 44 year old male?
I’ve been distancing myself from most people for about 10 days now and I’m going to focus on looking after my immunity with high dosage Vitamin C, Zinc and more.
Cheers again.
Thanks for the question... I haven't seen any clinical data on mortality rates of individuals with Cerebral Palsy with COVID-19 so I can't give you an evidence-based answer in that sense. With that said having discussed this with a couple of colleagues today our consensus was that we don't think someone with mild CP who is able to walk unaided and exercise should be at higher risk.
As to the penicillin allergy. I wouldn't worry about that, there are lots of other effective antibiotics still available to treat any bacterial pneumonia which might develop should you develop COVID-19.
With that said I would, as ever, urge social isolation, distancing and handwashing.As the Americans say to the veterans, “thank you for your service sir”
My question is probably more complex than I think but here goes
Viral loads and contagions. How does it work with this virus. We know that there are drugs for example that can suppress viral loads of HIV to levels that make it virtually not transmittable. What is it that makes this virus so contagious? Is it it’s ability to replicate itself? Or have I oversimplified it?
LOL! You were right that any answer to your question would be very complex and nuanced. At a basic level though different viruses have different levels of infectivity and we have just gotten quite unlucky that SARS-CoV2 combines quite high infectivity with a high R0 and quite a high rate of causing severe infections when it infects people. This basically gives it a high chance of overwhelming critical care resources. When this happens death rates could be reasonably expected to rise from roughly 2% ( when the system has enough critical care resources ) to 10% ( when the critical care resources are overwhelmed ). If you run the numbers from Italy you can see that their number of dead has been slowly but surely creeping up towards 10%.
@ Dummy_crusher
Thanks. I'll pass you over then.Is there a reason for the high mortality rate experianced in Italy to date as compared to other countries?
Discussing it with colleagues we think there are four main factors.
1. We don't yet have proven, effective treatments to beat the virus back in those who present with it.
2. Italy has a proportionally high number of aged individuals - who have higher mortalities.
3. They didn't react quickly and aggressively enough in terms of aggressively imposing social isolation on their citizens. They ratcheted it up gradually and by the time they got serious about it their numbers were destined to climb so high that their healthcare system got overwhelmed.
I think it is really encouraging that their numbers aren't breaching 500 dead a day yet. On a worst case scenario I had thought they could be breaching 1,000 dead a day by now so clearly their lockdowns have had some impact but they needed to take the Singapore approach ( mass testing, harsh, massive enforced social isolation) much earlier to prevent this death rate. They didn't and so they'll likely end up with somewhere between 8,000 to 10,000 dead by the end of the month - it could be a bit less if their lockdown from two weeks ago kicks in but I think that any [positive impact in Lombardy will be negated by rising cases and deaths in other regions of Italy where they didn't take it as seriously until much more recently.
4. The healthcare system in Lombardy has been overwhelmed and in that region it seems their death rate is at 10% already and has been for some time - this is the sign that their critical care systems have been overwhelmed.
I talked about mass casualty ethical triage previously and mentioned "black tagging" people as not suitable for any treatment. Channel 4 News is, in my opinion, providing the best news reports on this. They had a very interesting piece in which an Italian healthcare worker spoke about their active black tagging policy. This shows you how overwhelmed they are.
Channel 4 News Link: The relevant section begins about 3:20 but watch the whole thing. It is striking.
Also note that none of the civilians with face masks are actually wearing them properly. If you freeze frame at 4:40 you can see two people with face masks ( wife and daughter of a COVID-19 patient ) both of whom haven't fitted the masks properly. They think they're getting protection but I guarantee you they will both come down with COVID-19 Essentially all they've done is wasted those masks.
At 5:25 the kids of the man being taken to intensive care are allowed to touch his hand before he goes into ICU. He's lucky enough to get a bed but their awareness of infection control is very poor. To be fair, they're young and almost certainly will have caught it before this but it hurts to see the lack of infection control measures evidenced throughout this video by the public in Italy.
To be fair when I started enforcing this in my clinic a couple of weeks ago long before the HSE was mandating it co-workers thought I was hysterical too. They've come around.
Remember, every time you don't socially distance or hand wash properly you, personally, are making this scenario from Italy more likely to happen in Ireland.The One Doctor wrote: »No questions, just thank you for your forthrightness, bravery and determination. If we ever meet, I will buy you a beer. Several beers.
LOL! In all seriousness there's only two things I'd accept as thanks:
1. People passing this info/thread on to others so they could become informed and change their behaviours and
2. If you really want to give thanks I treated a lot of survivors of rape in A&E when I was a junior doctor. It left an indelible impression on me as a young male and so ever since I've supported the Rape Crisis Centre. Maybe drop them a donation in the name of Pseudonym121 ;-).
a) It'll help a very worthwhile organisation and
b) It just tickles my funny bone to think of how confused they'll be about any donations coming in with that nickname attached ;-)https://journals.lww.com/ajg/Documents/COVID_Digestive_Symptoms_AJG_Preproof.pdf
————————————————-
Conclusion: We found that digestive symptoms are common in patients with COVID-19. Moreover, these patients have a longer time from onset to admission and their prognosis is worse than patients without digestive symptoms. Clinicians should recognize that digestive symptoms, such as diarrhea, may be a presenting feature of COVID-19, and that the index of suspicion may need to be raised earlier in at-risk patients presenting with digestive symptoms rather than waiting for respiratory symptoms to emerge. However, further large sample studies are needed to confirm these findings.
—————————————————-
There are some reports that Gastro problems (like diarrhoea) can be an advance warning and in a small study of Hubei patients, just under 50% had this as their primary symptom. Have you heard anything regarding this or is there any sign that this has been a symptom from what you have seen thus far?
Thanks for answering all these questions, it really helps...
Fortunately we have a fox what used to be Professor of Cunning at Oxford Univesity but has moved on and is working for the UN at the High Commission Of International Cunning Planning working on this. ;-)
Yeah, gastro problems definitely seem to be more common than with the common flu. I know there is talk about this as a marker of potential severity of illness down the road but I don't consider that proven definitively by research yet. It is an evolving situation so that answer could chance a month from now.
Either way though you're just better off focusing on social isolation, distancing and hand washing.I'm a bit confused about the advice regarding hygiene/social distancing - HSE website says masks are unlikely to be effective for healthy people and seems to advise against gloves, but you reckon it's irresponsible to go to a supermarket without gloves and masks? Also, if we're worried about touching surfaces in a supermarket then what about the things we buy and take home? Should we be disinfecting packaging? Thanks.
Well the answer is nuanced:
1. Masks tend to be useless for the public because they don't know how to use them properly and so don't get much if any protection from them. Social isolation, distancing and hand washing are much easier for the public to actually do properly.
2. I think that if given the option one shouldn't go to the supermarket at all. One should just have food delivered. I haven't set foot in a supermarket for about a month now. I've moved to only home delivery.
3. If, however, you are determined to go to the supermarket in person then, yes, I'd suggest taking all the precautions you can... with that said there's no point wearing a face mask unless you've watched videos outlining how to properly put them on, fit them and take them off ( I provided several links for this in this thread ). Otherwise you're just wasting resources that healthcare workers could use.
As for the things you take home... That's a really good question. I use the following procedure and even then I think it isn't perfect but it is about as good as I'm going to get without professional equipment.
1. When a food delivery comes in I have an area set aside for the delivery to be dropped to. I now assume that the hallway it passed through and the room it is dropped into are infected. I wear a mask and gloves during the delivery process.
2. I don't go into the hallway or room it was dropped into for 3 hours without wearing a mask... Ideally I just don't go there at all. This is to let droplets settle.
3. I now retrieve the frozen goods, wipe them down with disinfectant wipes and place them in the freezer.
4. Non-frozen goods are wiped down or placed in a UV light steriliser ( for baby bottles ) as that has a decent chance of breaking down viruses etc and is a quick and easy thing to do with ready meals, keys, swipe cards etc which can be contaminated when out and about. I don't think is a perfect solution at all but in a home environment it is a a cheap enough intervention ( disinfectant wipes are cheap, gloves are cheap and the mask I wear is an N99/FFP3 reusable half face mask - the UV sterilisers can be bought on Amazon for 40 Euro to 100 Euro depending on size etc ).
5. Other jars, bags of pasta, rice etc are wiped down with a disinfectant wipe and then popped into the UV steriliser for about ten minutes at a time. Sure it might take me 6 hours to process a delivery but 3 hours of that is just leaving it sit in a closed room and then the next three hours is processing the delivery for storage and mopping the floor with bleach and cleaning other exposed surfaces.
It isn't perfect by any means but:
a) it only cost me the cost of the UV steriliser and
b) I only get a delivery every fortnight
c) I can have the radio and TV on during the process so am not missing out on any news etc. I don't make phonecalls during the time as being distracted is how mistakes happen.
Is it overly cautious? Well, it certainly is on the extreme end of preparations but, then again, I figure I have between 15 to 20% mortality if I catch this and if I survive I can expect to live maybe another 30 years so spending a few hours cleaning once a fortnight and looking like a weird survivalist prepper to the deliveryman is a price I'm prepared to pay. ;-). Additionally I have a responsibility to my patients and colleagues to stay as well as long as possible in order to continue providing care. Even if I were to die from this dying 6 months from now vs dying a month from now is 5 months of useful work supporting patients and staff. That's well worth it.
Obviously once a vaccine rolls around, even an experimental one, I'll take it and be delighted to abandon all of these precautions.
If there is interest in the routines and habits I'm trying to instill in myself to minimise the chance of bringing this into the home I would be happy to outline them in a post. Let me know.... you can't rely on yourself remembering these things willy nilly. You really need to think it out and have either a mental or written checklist. That's how we do things in surgery and when dealing with infectious or immunocompromised patients. We're learned that checklists work.My wife finished chemotherapy 6 months ago, and had a splenectomy 3.5 years ago.
We understand she is in an at risk group.
Are there any extra precautions that we should follow - over and above the guidelines for self-isolation?
No, I would just stress that you need to really practice self-isolation... not self-isolation with the occasional chat across the fence or when I run into someone on a walk. Self-isolation means staying at home for the duration with only essential trips out ( for food or medicine but even there if your pharmacy will deliver then have them deliver). I'm picking up some medication tomorrow and I'll be wearing the latest Spring Armageddon look - gloves and facemask - when I go. With that said I am trained in how to properly use the gloves and facemask ( privately purchased, not from HSE stores ) which is why I say I don't think a facemask makes much difference for most people - as they don't get any benefit because they put them on, fit them and take them off incorrectly.My sister smokes but had leukemia when she was a child. ( not had problems or check ups in decades). She works in a hospital up north and when I asked her if she had spoken to a doctor about her risk factor she said she didn’t see it being a problem. She’s also refusing to buy these personalized masks they are offering. Would a person who has , I think, fully recovered from this illness theoretically not be anymore at risk then the average person? I appreciate you cannot give medical advice here, I am just wondering how insistent I should be with my sister that she should talk to a doctor regarding her risk profile, especially while she’s working in a hospital....
Yeah I can't really give individualised advice because I don't know the full situation but my compromise is that I can talk about the generalities which seem to apply and then suggest what I think would be a reasonable course of action.
I would imagine that a fully treated and in remission cancer from many years ago for which she isn't still taking any chemo shouldn't put her in a high risk category because, essentially, she had an illness, treated it and now doesn't have it any longer. With that said a lot would depend on individual factors - some jobs in the health service are lowish risk, some are very high risk and I'd expect 100% infection rates in some roles.
I think it would be smart for her to talk to a doctor regarding her risk profile given the fact she works in a hospital. With that said I'd expect they'll say that a resolved cancer with no ongoing treatment doesn't put her in a higher risk group. So, I expect it'd be good news.Fluorescence wrote: »Thank you for taking the time to answer the questions, and for continuing to work despite being at considerable risk. This really is a war.
I work in the veterinary sector. Many of our clinics and hospitals have ventilators. In the UK, the AHT is compiling a list of veterinary ventilators and liasing with officials to coordinate their potential donation/use in the hospitals in the weeks to come. I don't know if the Irish bodies are aware that these facilities may be available to draw upon?
It's not a standard piece of kit in every hospital but there are many around, which may be worth investigating.
Aside from ventilators, is there anything veterinary staff in particular can do to assist in the coming crisis?
Well, I think you can do two main things:
1. Contact your representative body and ensure they are in contact with the government about these ventilators. It does seem to me that the HSE has been pretty good about scouring the country for ventilators and it seems to me we have roughly doubled the number of usable ventilators ( from private hospitals, converting ORs and buying more ). That's going to have a huge impact on keeping people alive. We still need more though so I think ANY ventilator going would be welcome. Funnily enough we make a large portion of the world's ICU type ventilators in Ireland so that'll be helpful.
2. Consider contacting the Ireland's Call website. If you know how to place lines etc then I could see there being a role for you and others doing minor clinical tasks which would normally be done by nurses etc which would allow them to be freed up for more crucial tasks.
It seems you understand this but it bears restating. Ireland is about to have a small to medium sized war, with all of the casualties that entails. Anyone who has skills in treating mammals will be useful because humans are just unusually hairless mammals with pretensions ;-). With that said I'm sure that if you aren't comfortable taking on a clinical role there will be a lot of roles in providing deliveries to the elderly during the cocooning phase etc.Hobgoblin11 wrote: »Is sex ok during this crisis or should we be avoiding that also?
When can we go back to this type of thing if it's not recommended?
Do you contact trace your partner?
Well I think having sex with someone you don't already live with is certainly increasing your risk. I'm not even sure this is a serious question but I'll answer it as though it is. I'm single and I certainly amn't going to be dating until either a vaccine is available or I've been infected and, hopefully, survive.
As to contact tracing... I assume that's a joke but if it isn't then I'd suggest that you can't know whether someone is infective or not no matter what level of contract tracing you plan to undertake. With that said people often put themselves in danger in pursuit of sex so I'm sure many people will continue behaving less than logically in this area going forward.I see that having high blood pressure is one of the risk factors. If you are on medication for it and your BP is now ok, is an underlying risk still there?
Yes but I would expect that well-controlled high blood pressure is less risky than poorly controlled high blood pressure. With that said even with well-controlled high blood pressure I would consider myself to be in a high risk group.Arlessienne wrote: »In your opinion, how high risk is someone (aged 40) with Inappropriate Sinus Tachycardia requiring 7.5mg bisoprolol daily and suffering fairly significant exercise intolerance? They are an ex medical scientist and looking to volunteer - is their risk of further burdening the health service if they get sick low enough to go ahead? It's impossible to get any response at the moment from gp or cardiologist. Obviously this would be just your theoretical opinion on this condition generally, without knowing full details.
Thanks for all you are doing both in the hospital and in spreading awareness here. Your posts are scary but I believe them to be realistic. Thanks for trying to get people to wake up to reality.
Thanks for the question. I don't wish to be difficult but there's no such thing as inappropriate Sinus Tachycardia. I think I know what whoever used that term meant though and I would think that this would qualify as Cardiovascular Disease and thus put them in a high risk category.
In terms of volunteering with the Ireland's Call initiative... There will be need for people taking on clinical roles and non-clinical roles. With the non-clinical roles some will be asked to present themselves to certain sites and others will be able to work from home.
So, even if in a high risk group and completely socially isolating at home I think there will be roles that this individually could do without increasing their risk of exposure one iota. If I were in your shoes I would encourage them to volunteer ( I think that's really helpful right now and everyone who can help out should ) but to do so in a role which could be done from home without them breaching their social isolation.
There are LOTS of young people in their 20s and 30s without any health conditions who should volunteer for patient-facing roles if at all possible. Some of us with health conditions need to put ourselves in the firing line because that's just where we need to be right now BUT I don't see any sense in this individual putting themselves in the firing line when there's an option to help out which won't increase their risk.
Obviously that's just a general answer but I hope you find it helpful.lillycakes2 wrote: »I am a nurse, I live with my mum who is over 70,self caring. I am not going near her, I am using just one room (my bedroom), with door closed, I am using my own toilet, my own cutlery and I just walk out front door when I go to work, she is not allowed to use this door , she uses the back door.i am not using any room in the house ,I am showering etc in work....
Does this sound ok to you ?.
Hi lilycakes2. Those all sound like sensible precautions alright. It seems there's a desire to have a post on how to prevent bringing infection into the home. I'll write an essay type answer up for that over the next couple of days but it definitely sounds to me like you're doing much more than most. There might be a few areas one could improve though through the purposeful establishment of a room to clean and change on entering or prior to leaving the house so that the rest of the house could basically be considered a "clean house". That's the approach I've taken -turning a spare bedroom into a changing area and taking off my clothes from work there and then cleaning my hands and showering on return from work. Once that's done I consider myself clean and then can just potter around the place with no concerns. When I'm going out I go into that room, assume everything in there is infected, change and then go out.
I'll write it up in fuller detail as I think there are a number of people living with elderly relatives who are concerned about this sort of issue and want to make reasonable changes ( which would have sounded utterly hysterical just a few weeks ago ) to make things as safe as possible.supermouse wrote: »Firstly, thank you for doing this AMA. Furthermore, thank you so very much for everything you have done to date and will no doubt continue to do well into the future to protect us all.
Why do you think we haven’t been put in lockdown yet? As we’ve all heard and seen, social distancing is working for some but so many are ignoring the rules. Mr Varadkar has access to the same data as you, is a medical doctor himself and is surrounded by some of the brightest minds we have in this country. Why are we delaying the inevitable do you think?
Stay safe. I truly mean that.
Thanks. This is part of my small contribution to this and I'll continue answering questions for the duration or until I'm no longer able.
I think that people, on average, are self-deluding and prefer to live with imaginary safety rather than real-world reality. It takes time for people's mentality to shift from their rose-tinted view of the world to the reality we now find ourselves living in. This is made worse by the fact that what scares me and others who understand viruses and epidemiology is NOT today's figures but where they'll be 1 month from now if we don't act now. People in general are very bad at visualising a future situation and acting now to prevent it. They look at today's situation and base their decisions on that --- you see this with climate change. People have really only started getting on board when current storms have undeniably become more frequent and severe --- even though we KNEW that would happen for at least two decades.
As to Leo being a medical doctor. LOL! If I remember correctly he went straight from internship into GP and from there into politics. I mean I was an intern and SHO at one stage too but God help us all if interns and SHOs are making these decisions. They're very much still learning. I see this with my own NCHDs whom I've been talking with about the epidemiology of this. They have a basic understanding but not enough to really get as scared of this as they should have been --- to be fair I think mine have been scared enough that they and their families took appropriate steps weeks ago because I sat them down and had some significant chats with them about how serious this was going to be and their responsibility to prepare in order to be of use to the health service and public going forward. I don't think too highly of Leo's insights into medicine - hell, I remember him as a GP trainee, I had occasion to interact with him professionally back then. He was fine but I wouldn't be listening to him on epidemiology right now. To be fair to him he hasn't made any claim that his medical background such as it was gives him any special insight right now. He has, as far as I've seen, stuck to the line that he's listening to the expert group. I am not a fan of him on a personal or elective representative level but I think he is managing this pretty well all things considered.
Anyways, the government has a public who just don't get it and moving them to where they need to be takes time. I think we are seeing that process in action. This reminds me a lot of how Singapore managed things with SARS back in the day. They tried gradually increasing restrictions etc too, realised it cost a lot more deaths and went straight to the full suite of measures this time. End result, they have this largely under control.
While I think we should have adopted the 2020 Singapore model from Day 1 I recognise that:
a) the resources and planning just weren't there and
b) the Irish people wouldn't have gone along with it... I think the public has had to go on a journey to understanding this was serious --- and even today there are really disheartening images of groups of people in town and shops etc.
Overall I think that going with the mass testing, contact tracing and delaying spread while building up ventilator and hospital bed capacity model is probably the best we could realistically do given the fact that Irish people just didn't have the SARS experience that Singapore had back in the day.I live with my elderly parents and I myself am on weekly benepali injections. When the government recommends cocooning, would I need to follow that recommendation as well as my parents? We live in the country with no family nearby so would need to be thinking about trying to put arrangements in place if necessary.
I think that if they cocoon and you are out and about then there's a significant risk you'll bring SARS-CoV2 home. As I said above I'll post about the steps you could take to minimise the risk of bringing that into the home.
But the basic point is that if one person in a home is going out then they certainly have a risk of bringing it into the home and should take significant measures to reduce that risk.
Right now the real countries to look out for are, IMO:
1. Iran - but that's pointless because they are not being honest about their figures.
2. Italy - this is where we'll see lockdown in a Western European country work first. This should then enable the Irish government to sell these measures to Irish people.
3. UK - they're our closest neighbour, are taking a different approach and should exceed 100 deaths per day 5 to 6 days from now. I think that will be a psychological benchmark for them.
4. USA - I think they're going to have a horrendous outbreak of this. I think they're going to make Italy and the UK look like nothing. The Federal response has been terrible and only local state and even university-level actions have been in any way effective there. I think their number of undiagnosed individuals actively spreading it currently is huge and their healthcare system is NOT set up to provide the socialised care a pandemic needs so structurally unless the federal government steps in they're in terrible trouble.
They'll show us the path out of this for us ( Italy ) and the worse (UK) and worst (USA) case scenarios we could have experienced if we didn't have the response the state has generated.
To their credit I keep hearing management tell us that "money is no object" right now and that if we need something which will improve outcomes then the money will be there. Obviously there's a lag time in ramping up production but at least the government in Ireland really is taking the attitude that it'll spend whatever it has to to save the most lives possible --- we just need you, the public, to do more social isolation. Right now you aren't doing your part and this will cost hundreds, possibly thousands, of lives in coming months.0 -
Join Date:Posts: 70125
Another reminder - this thread is for the AMA answers only. Questions should only be posted in this thread0 -
A genuine question, and I know it might be impossible to answer, but do you foresee this going on for a few months or are we looking at a new normal well into 2021?
I've been on record since I first starting posting about this 3 or so weeks ago that we will still be talking about this in March 2021.
We will be talking about this until we get a vaccine and even then we'll still talk about it because by its nature I expect it will generate enough generations of infection to mutate into different strains. I expect ( but this isn't proven, just my expectation based on my understanding of how new strains develop ) that COVID will become a seasonal thing like the flu and generate COVID-21, 22, 23 etc and become just like seasonal flu except much, much deadlier to the elderly. It will probably drop worldwide life expectancy by a few months to a year over the next decade.Arlessienne wrote: »Thanks so much for your response. It was very helpful. I will pass on your advice about volunteering for a role with no or little contact and he will hopefully eventually get a specific response too from one of his doctors to be safe. (IST is the official diagnosis written in medical reports from a cardiologist specialising in electrophysiology and was deemed to be a type of SVT and possibly a form of dysautonomia or SA node malfunction.)
Best of luck and thanks to you and all your colleagues.
Hi, thanks for the reply. I can see i was unclear when I said there is no such thing as inappropriate sinus tachy. Sure it is a term that is used but it doesn't describe underlying pathology. It can be caused by anything from drinking too much caffeine to a serious life-threatening disorder of the electrophysiology of the heart. That's why I was saying there's no such thing --- although I can see that wasn't as precise as I should have been.
So, now you're saying that IST actually represented either the cardiac pathology of SVT or SA node dysfunction. Either SA node issues or SVT are cardiac issues. I think the best way to deal with this and play it safe and say - "Well, if I have a cardiac diagnosis then I'm going to assume that puts me at higher risk". Other doctors might differ.
I am unaware of any evidence which says SVT and A Fib are not associated with high mortality in COVID-19 so I'd prefer to play it safe and assume they are higher risk. If that evidence evolves or someone can post a link to such a paper I would obviously defer to it. Our knowledge base re: COVID-19 is continuously evolving.
Damn, I just deleted the answer I'd written to the next question. here goes again.
We simply don't know why some people incubate for 5 days or 14 days. We also don't know how long they are infective before they develop symptoms although most people now think it is at least 12 to 24 hours. For the test to be positive enough viral RNA needs to be on the swab to be amenable to PCR. But we don't know how long that takes and if that varies from the 5 day incubators to the 14 day incubators. We are still learning a lot about this virus.up for anything wrote: »Based on our figures today, 20th March, and the lack of proper social distancing going on, what do you think our best, medium and worst case scenarios are going to be regarding deaths?
Good questions albeit I think the answers may not be re-assuring. I've explained previously that in this sort of situation one method is to come up with 9 scenarios - Best, Middle and Worst and then divide each of these into Optimistic, Reasonable and Pessimistic.
I'm on record previously as stating that the best case scenarios I foresaw for Ireland over the next year were as follows:
Optimistic Best: 2,000 Dead.
Reasonable Best: 5,000 Dead.
Pessimistic Best: 10,000 Dead
Optimistic Middle: 20,000 Dead.
Reasonable Middle 50,000 Dead.
Given the steps we have taken I don't see us exceeding a reasonably middle case scenario anymore so I won't go into the worst case scenario numbers. I'm sure the government has even better estimates. These were my estimates created when I began researching this 3 to 4 weeks ago. I think they're still valid although we're now more likely to be in best case scenario territory than middle and worst case like we were 4 weeks ago.
The proviso for the above is that IF we got an experimental vaccine in good numbers by September 2020 then you could see those numbers fall by 80%. The reason is that if this follows the Spanish flu modality then we could expect a massive spike in deaths in Q4 ( I believe roughly 80% of all Irish deaths over 1918 and 1919 occurred in just 8 winter weeks in 1918). Is it guaranteed to follow this pattern? No, but I think that assuming it will isn't unreasonable. It could still be wrong though.up for anything wrote: »Are there going to be enough ventilators, do you reckon, for say the medium case scenario? I assume, probably wrongly, that as we are a manufacturer of them we may get first dibs on them.
No, no there won't be. The state has done amazing things to increase the numbers of ventilators, staff and beds but the public has NOT done its part in terms of social isolation and distancing and, as such, the public has condemned many more to death than were unavoidable. Well done guys.
Medtronic makes a large number of worldwide ventilators seemingly. They have boosted production and will boost it more. My understanding is that what they would have produced normally is already bought by other countries and it would be very foolish for the Irish state to requisition them - we'll need other countries soon enough and they'll remember if we screw them over and return the favour. I'm sure we've negotiated/strong-armed quite a good proportion of the increased production though - and this would be more tolerable to other countries.up for anything wrote: »Are patients who are within some hours of inevitable death actually in any sort of condition to say goodbye to family via phone or iPad like I've heard they've been doing in Italy?
If they're tubed and sedated then they're not. If they are more conscious then a remote goodbye may be possible so long as staff aren't overwhelmed.LadyMayBelle wrote: »Thank you so much for your advice and info, as well as your dedication. I'm glad you gave example of how you managed food delivery and wiping down items, as I worry about this as well as good intentioned people leaving items and bags of things at people's doors, esp elderly. I made clear in another thread that it's not about stopping kindness but a need to be mindful that more harm could be done than good? Once proper measures are in place then it's ok..ish.
Would love your broken down list you referred to..we would have been chuckled at for being preppers but took a lot of advice from your posts. Thank you.
Well, I actually enjoy watching those prepper shows for a laugh because I find their risk assessments and planning so one-sided and often missing huge issues which render the whole thing impractical. I've never gone in for that... but, like I said, when I figured out the stats behind this when I read into it 3 to 4 weeks ago I knew I had to prepare... and so I did and persuaded my family to also.
I'll write something up today/tomorrow re: dealing with food deliveries...Funsterdelux wrote: »Howdy doody Pseudy,
I was up on scaffold there starting to get the battens ready for slating the back of my cottage, the east wind is eating the face and hands off me. It got me thinking, with the measures of social distancing/isolation in place for months perhaps, other viruses such as the cold and flu would also find it hard to spread(i know we're going out of season). Would this have a positive or negative effect on our collective immune system? If a majority of us dont catch sars cov2 and other viruses, when/if things go back to normal would we be more at risk from getting a more severe cold/flu?
The question always sounds better in my head, anyway thanks again and good luck!
No worries. I don't think that the impact of social isolation on flu will have much impact on the flu season 2021.If suspected cases have to wait days for a test and,as a result, test negative because theyre better what is the point in testing if not testing for antibodies at the same time?
Surely these tests should be allocated to people on the list with symptoms.
A work colleague of mine was sick for 2 weeks
GP booked a test on Monday and still waiting. Says he's feeling better now and wonders should he give his slot to someone else on the list. Thanks to you all.
I'd still go for the testing as enough RNA might remain to give a positive test and re-assure the individual that they are now immune to the current strain of SARS-CoV2.
I think the delays in testing and overly strict testing criteria will both change as more tests are available and more lab capacity is diverted to COVID-19 testing.
Yes, you're right that an antibody test would be very useful but, in the meantime, we use what we have because widespread testing and enforced isolation has been shown to be hugely beneficial in preventing spread.Hello and thank you so much for answering questions during this time. My dad found out he needs a triple Bypass a week and a half ago. He is meeting with the surgeon on Monday. He is 75 and will be tested for Cov 19. My question is, in your opinion, could I visit him in relative safety before and after the operation while keeping 6ft between us, wearing gloves and mask? I am in good health, no symptoms whatsoever. I do have children. I am extremely close to my parents and other family members have visited, keeping their distance. I am torn between fear of passing something on and the negative mental health effects not seeing them is having. Many thanks Fjortal
I think that elective surgeries like that won't go ahead soon.... I'm unclear if you're saying he is due to be operated on on Monday - in which case it might still go ahead - OR if he is meeting with the surgeon to discuss surgery at a future date - in which case I would expect it to be postponed for the foreseeable future unless he would die without the surgery.
If it were me I wouldn't visit him. I'd use skype to videocall. I haven't seen my own parents except through a window or skype for about 3 weeks now. You have to balance the risks vs benefits yourself but heart surgery is a significant operation and putting him at extra risk seems madness to me - especially when we have skype. Sure it'll be a low level of extra risk but I just don't think it'd be worth it if it were my father.
You'll have far more negative mental health effects if you infect him with COVID-19 and he dies.
That'd be my attitude but you know yourself and your parents in a way I never could so you'll need to balance that yourself.Potentially wrote: »Firstly, thanks, no words could say it enough
Secondly: I am a single Mum with 12yo. Ex wants to continue contact, he has just collected her and has gone off for the day. He has been working as a salesman to pharmacies and has continued his normal socialising routines, with his new partner (nurse who home-cares for newborns) and others home recently from abroad....
I have been really careful to keep social isolation but is all that down the drain now?
My elderly parents and aunts rely on me; and if I get ill, there is no where for my child to go.
Please advise.
I can't tell you what to do in your situation but your ex's behaviour seems to be begging to be infected. If he continues having access to your child you should assume she will be infected also and from her you'll be infected.... and you could pass it on to whomever you have contact with.
I've heard many separated couples are fighting about this sort of thing when one partner isolates and the other doesn't. I think that is a tough situation to find oneself in.Notsomindful wrote: »Thanks for all you are doing.
My local testing centre is a drive through centre.
I have been referred for testing awaiting appointment.
Can I walk to test centre- as I dont have access to a car and dont want to risk spreading it to others unnecessarily like taxi drivers etc...
Yes, just be very careful to stay more than 2 metres from anyone if at all possible while on the way there. The risk of passing it to others outdoors if you pass by briskly and stay more than 2 meters away is low. Not zero, but low.RobbingBandit wrote: »Thanks for taking the time to do this.
I'm a diabetic I've just had my next couple of appointments postponed indefinitely I am currently dealing with several complications including foot and eye issues which require routine care and can turn nasty I am unable to contact anyone in the departments so far and really don't want to find myself going to a&e.
In short what is happening to patients with ongoing chronic issues in this current climate is my question.
I think we're doing our best to keep services going for our routine appointments but in a crisis like this routine care will inevitably suffer.
One of the unmentioned aspects of crises like this is that you only ever hear about the people who died from the crisis illness ( e.g. ebola, COVID-19 etc ). You don't hear about what epidemiologists call "excess mortality" which is those people who died in excess of the normal rate for that time of year.
So, let's say 100 people a day die in Ireland normally in April and this year we have 20 COVID-19 deaths per day in April but when we pull all the figures we find actually 130 people a day died in April. In that situation 30 additional people died every day due to the crisis, 20 from COVID-19, 10 from other illnesses who would normally have been saved but couldn't be because the health service was overwhelmed.
In Italy they are reporting an increase in death rates from cardiac problems and other issues even in patients who don't have COVID-19 because where it used to take 8 to 10 minutes to get an ambulance out to a heart attack it now takes hours - by which time many are dead.
So, that's grim.
In your case I'd try to make contact with the Public Health nurse or your GP if you can't reach your specialist. I'd also redouble whatever efforts you are making to manage your blood sugars etc as well as possible yourself.
So, in short we'll do our best but, yes, you won't get the quality of care you're used to and the more selfish A***oles go around not socially isolating and distancing and handwashing the more medical and mental health services will be overwhelmed, the more appointments will be cancelled, the more surgeries will be cancelled and the more people with ordinary health issues but not COVID-19 will die. Congratulations Irish public.Airyfairy12 wrote: »Hi I just have a question about coronavirus symptoms. Do they come on suddenly like in the case of a flu were you all of a sudden feel unwell or do they come on gradually, do you feel like youre coming down with something for a day or two before symptoms become obvious? Are swollen lymph nodes in the neck common with coronavirus like they are with cold and flu?
Thank you so much for taking the time to answer questions.
It is really quite variable. A lot of doctors have gotten it over the past week and many of them have described really rapid onset of symptoms. Some have literally sat down to dinner fine and been unable to finish the meal because they've become unwell.
Others report a gradual worsening of symptoms over days.
So, I think it varies a lot and there isn't a one size fits all presentation.
As to lymph nodes. I haven't heard much about swollen lymph nodes being a significant sign in COVID-19 presentations. With that said I think we're learning more all the time. Hell even today they're beginning to coalesce around anosmia etc as a significant symptom and that wasn't on anyone's radar in Europe a week ago. So, it is an evolving situation.
Ok, hope that was helpful, I think I'm caught up now.
Edited to clarify the answer for SVT/ A Fib and make it clear that the answer was based on "erring on the side of caution" in the absence of evidence of either issue not increasing the risk.0 -
@ SilentRunning.
Controlled A Fib is a chronic cardiovascular condition and chronic cardiovascular conditions are known to increase risk of mortality.
@Fishy Fishy
Re: having complete faith in your ability to survive it... You shouldn’t. Younger people are dying in Italy and the US. About 20% of recent deaths in the US were below 65 years of age.
Re: Asymptomatic spread. It is all about viral load vs presence of symptoms. It seems that many people with COVID-19 have a period of time where they have a high viral load in their throats/nasal passages prior to the onset of what they recognise as symptoms and so can spread the virus to others while being “asymptomatic”.
No, my level of preparation is not common. WHen I read up on it about a month ago now and decided that this was going to be a huge problem none of my colleagues outside of, perhaps, infectious diseases and public health seemed to be as worried as I became. They certainly didn’t buy in the masks, gloves etc which I did and urged my family to do.
Re: survival rates on ventilators. Read this and prepare to despair.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30110-7/fulltext
86% of those who required invasive ventilation died and 79% of those who required non-invasive ventilation died. So, basically 42 out of 52 ICU admissions ideas. That’s one hospital in Wuhan and small numbers but even with ventilation they were looking at over 80% mortality for those admitted to ICU.
It sounds like the numbers are even worse in Italy but they’re too busy treating patients right now to be writing peer-reviewed papers.
It is GRIM and everyone going out and about and not rigidly socially isolating or distancing is actively adding to the death toll in Ireland.The One Doctor wrote: »Does the current low number of deaths from CoVid 19 in Ireland give you any cause for hope about this pandemic?
Thank you for your stalwart work.
No, given the public’s failure to socially isolate and sufficiently socially distance we are still on track to have thousands die over the next year, possibly over ten thousand.Hi
I’m a dentist. Like most of my profession I’ve shut my practice due to safety issues.
Unfortunately the chief dental officer made a statement that we’re to work as normal despite not having appropriate PPE.
Her advice is plain wrong. I don’t want to be a super spreader ( because I don’t have PPE) , nor put my staff or our families health at risk by remaining open. However I also feel a duty of care to my patients.
The hse needs to order all dental practices to shut down. We might save a tooth but loose a life!
Hi. I’m sorry to hear your difficulties. Yes, I was being given advice/instructions by the HSE a couple of weeks ago which were not in keeping with the objective reality of what the risk was. I ignored them and enacted precautions which the rest of the HSE moved to some time later.
When instructions from on high don’t make sense it is time to take one’s own authority and do what you know is right. I may get fired for it but at least I know I tried to protect my patients and team as best I could.
You also have to bear in mind there isn’t enough PPE so that plays a part in telling you you don’t need it. If they told you you needed it they’d then have to tell you they had none for you. Cynical, moi? To be fair nowhere in the world has enough PPE so just like in some wars the first wave or two of healthcare professionals are going to the front lines without the right equipment. They are therefore suffering very high infection rates right now.
Is that a failing? Not really, very few people saw this coming a month ago and one cannot really blame them as this is really an outside context problem. Very few humans or organisations cope well with these.
We are doing OK as a country so far. Could have done better of course but we are doing better than a lot of places. At this point the public is letting us down massively with the cavalier attitude in many areas.0 -
If you’ve had the vaccine for pneumonia would this protect you from pneumonia if you get Covid-19.
Not significantly no. Streptococcal Pneumonia is what this vaccine protects you from. Not all pneumonias are caused by streptococci and it isn't, to the best of my knowledge, a major contributor to the bilateral interstitial pneumonia people with COVID-19 often die from ( they die from other complications also of course ).
TLDR: No.begbysback wrote: »Given that deaths can be kept at a minimum by early diagnosis and treatment, are you guys lobbying for this, or just waiting at the doors of hospitals for critical cases?
Where are you getting this from? There aren't any validated treatments which are widely available beyond attempts to treat complications and/or support people with oxygen/ventilation until such time as oxygen and ventilators run out.
You assumption that there is a validated treatment which changes the course of illness if someone is diagnosed early isn't where medicine is at right now. The Chloroquinine and azithromycin combo is in a single small study which could have numerous confounding factors.
I think your assumption re: "early diagnosis and treatment" is incorrect, unfortunately, at this stage. Once we have a validated treatment then that could chance but we won't be in that position for weeks or possibly months and that's going to be too late for the people who will die in the initial peak in Ireland over the next 2 to 3 months.Notsomindful wrote: »Thanks for link.
That's reassuring for all of us who dont have access to a car/dont drive and dont want to risk.infecting others.in taxis/ high risk themselves...according to the hse, we" may be tested at home".
So we may not get tested at all.
Woohoo.
Absent a validated treatment the benefit of testing lies more in contact tracing and you knowing you must self-isolate. It doesn't benefit the individual hugely as there isn't a validated treatment which alters disease course and outcome yet.
So, just assume you're infected if you have those symptoms and stay at home.
It is dangerous to just make unwarranted assumptions about treatment evidence, availability and efficacy. We really aren't there yet. Everything will be thrown at this and weeks and months from now we will know what does and doesn't work but for the next several weeks to 2 months our best defence is the public socially isolating, distancing and hand washing.
Unfortunately you're doing a piss-poor job of it. I was delivering supplies to my parents today and there were large groups of people out and about chatting to eachother and not observing social isolation at all.0 -
Thanks for doing this OP, first thread I’ll check anytime I’m on now.
I’ve noticed a change in your tone and attitude towards the public over the past few days (not saying it’s unwarranted btw). Do you find yourself overwhelmed already with the workload and job ahead or do you feel it’s more your own personal anxiety about what’s to come? I’m trying to gauge what of this is based on your actual day-to-day work/lived experience and what is (educated) worry.
On a similar note how do you compare your own state of mind to that of the colleagues you’re working with on the front line: are you one of the few preaching concern or are the majority of frontline workers freaking out about the public too?
My attitude is coming from simply seeing so many people out and about standing within 18 inches of eachother and having "the chat". Obviously a lot of people are taking it all very seriously but many others are just behaving in a manner which ensures easy spread. I've had to tell a number of people to stand back when they have come within a foot of me when out and about.
I can't talk for everyone but I don't think any doctor or nurse is happy to see people behaving in a manner which causes this to spread further.Nonoperational wrote: »From reading your posts I suspect I know what speciality you are in but I appreciate you don't want to answer that publicly. I am heavily involved in GIM and have already completed numerous covid shifts in ED and have seen nearly 100 patients ?COVID. May I ask, will you actually be seeing COVID patients during this and be involved in their management?
I appreciate you not wanting to let people know your speciality but could you at least clarify if you are GIM/Surgery/Psych etc. A broad category. Just so people have some context.
Thanks
Hi, fair points... and I saw this before the edit so I'll address that as well.
I've always been clear that:
a) My attitude is maximum caution with this and
b) that i can't give individualised advice for the reasons you mentioned before the edit but that where possible I would give a general view if I felt that was reasonable.
When someone says... I have cardiology problem A, should I be more careful? I see it as follows:
A) There might be evidence that it is absolutely high risk - point them to the relevant article or graph and say - here's the scientific consensus. There might not be evidence one way or the other. At that point one has three options:
B1. Sorry, no idea whatsoever until the meta-analysis comes out, won't even extrapolate slightly. This doesn't really help someone who has been unable to reach their treating team
B2. Since it isn't obviously high risk I guess it must be low risk - we are learning about this all the time and things we thought we knew one month ago are now known to have been incorrect. I'm sure we'll know more about it 1 month from now and some of our knowns will change and many of our unknowns will be clarified. Things we think aren't high risk now may turn out to be high risk down the road.... and vice versa.
B3. Since it isn't obviously high risk or low risk the safest way to behave would be to assume you're high risk. If this is wrong then someone may worry a little additionally unnecessarily. If this is right it could prevent them being infected and having a significantly sub-optimal outcome.
I've been very clear that where there is evidence I'll always defer to evidence but where there isn't strong, clear evidence one way or the other then I'd prefer to err on the side of caution. I think that is more helpful than just saying - since there isn't a meta-analysis on the subject I won't answer. I don't claim to have absolute knowledge but I do know how to err on the side of caution.
Are you saying that there's strong evidence that SVT or A Fib don't constitute an increased risk of mortality in those infected with COVID-19? You may well draw the line differently than I and if you do I'd be more than happy for you to pipe up. I am absolutely not trying to hold myself out as the font of all medical knowledge. That would be ridiculous. With that said pointing people to scientific evidence where possible and urging maximum caution where things are less clear is, I believe, a reasonable course of action. Don't you?
If not I'd be happy to have a discussion with you here or via PM as our schedules allow. No-one should slavishly believe what I say but I think there's a lot of information which is just blindly false out there and someone who is trying to give scientific evidence where possible and erring on the side of caution where evidence is less clear is a helpful contribution, IMO. You can of course differ and I'm open-minded enough to be open to persuasion.
As to the category... As I said, I'd rather not because even broad categories really lessen the parameters. I'm not forcing anyone to believe me or forcing anyone to do anything. I'm just trying to give evidence-based advice where possible and erring on the side of caution where there's less evidence.
So much is being learned about COVID-19 at such a rapid pace that no-one can keep up with everything. You may be aware of something I'm not. If you have better knowledge/evidence I'd be very happy for you to post it and help people. I'd have no problems with that.
With that said... I hear you about the shifts and wish you the best.
I've read back the A Fib/ SVT answer and edited it to make it clearer that the answer is an "err on the side of caution" in the context of A Fib and SVT being cardiac conditions so why take the chance... as opposed to "there are multiple meta-analyses which prove this definitely with a P < 0.0001 and a significant effect size". As always, the best solution is to have a chat with your treating cardiologist --- but in the meantime I think it is prudent to be extra-cautious until and unless your own treating cardiologist tells you that there's no extra risk in your, individual, case.apologies if this has already been asked.
it's horrible hearing the figures of people who may die from this virus but especially the fact that healthcare workers in our hospitals will also die, are all healthcare workers at risk due to their high exposure or is it the same as the general public, older with underlying conditions?
You're going to have different levels of exposure based on the different national and local situations. E.g. in China about 4% of cases were healthcare workers. In Italy it is over 8%. A lot of that may be down to the relative lack of PPE in Italy.
That's risk of exposure. Risk of mortality will largely come down to pre-existing medical conditions. There is some evidence out there that healthcare workers have increased mortality but I don't think that evidence is solid yet. It may prove true but I don't think it is quite at the necessary level to say it is certain yet. With that said if you have hundreds of thousands of healthcare workers become infected and even if only one in a thousand dies then the sheer numbers of infected add up to a large number of deaths.Do you think the number of cases so far is an accurate number? Also, is there a shortage of testing kits as 2 members of my family have waited 6 days after being referred for testing due to symptoms and underlying conditions and are still waiting. Thanks for your time and effort in this thread.
No, I believe it is quite openly admitted that there was a lack of testing kits which resulted in very stringent criteria being set for testing --- so stringent that a lot of people who may well have had COVID-19 didn't meet the testing criteria. This isn't negligence, it is just what happens when a disease blows up like this.
Availability of testing kits has improved significantly recently. The issue now is building the capacity to actually do the tests - that is low but is being increased every day. It will take time to clear the backlog and then engage in really wide-scale community testing.0 -
Advertisement
-
Sorry, I think I overlooked two questions somehow.Hi Pseudonym121,
Thanks for doing this. It's very informative and thought provoking. Stay well.
My questions is regarding suppressants (not sure if that is the right term) like cold and flu medications/remedies. I used to typically get a couple chest infections (with harsh chesty cough and perhaps sore throat and sometimes fever) a year. For the last few years I find that at the onset of symptoms if I take echinacea capsules regularly I can usually hold it at bay and after a few days I am back to normal. Where I have let it get deeper I would add astragalus to help clear it up. By the way, I'm not advocating the above in any way, shape or form as regards Covid-19.
Could the use of any of the above remedies by the general public cause problems by perhaps masking the Virus (reducing the symptoms and as a result people not looking for testing or being less cautious)? I think I read somewhere that some products had been banned in China for this reason. Possible fake news of course but perhaps you have better knowledge of this.
Would you have an opinion on this?
Sorry if it's not really relevant.
Anyway keep up the good fight and take care of yourself.
If in doubt I think you should ask your GP or respiratory specialist as that advice might vary depending on underlying medical issues. It has a quite a broad range of answers depending on underlying issues, sorry.Fleetwoodmac wrote: »Is there any truth in WHO giving directives regarding taking zithromax and chloroquine as prophilacs for covid?
Not that I've heard of. This appears to have been a very small study. Colleagues in the US have messaged me today with several messages from doctors using this combination to little effect... but Trump has run with it and so it is in the media.
It may end up being effective but I do not believe the evidence base is there to say that yet.Thanks for doing this and two questions if you don't mind:
1. My daughter works in a pharmacy and I fear for her health from additional exposure and then surely that impacts on the household's effort of social isolation, being made somewhat null and void. Should we be taken any additional measures?
2. The UK only reported 7 deaths today. A long way short of the daily 100+ prediction. Is this from lack of true testing numbers or signs that things are not as bad as feared?
Hmm... 7 Dead? I think it has been running quite a bit higher than that recently. Here's a good site which allows a breakdown of cases, mortality etc by country. Here's the UK page, scroll down for their daily number of deaths.
https://www.worldometers.info/coronavirus/country/uk/
They've had over 30 deaths a day for the last five days by my reckoning. Unfortunately I think it is only a matter of time ( just under a week probably ) until they have 100 deaths per day. It is very sad.0


This discussion has been closed.
Advertisement